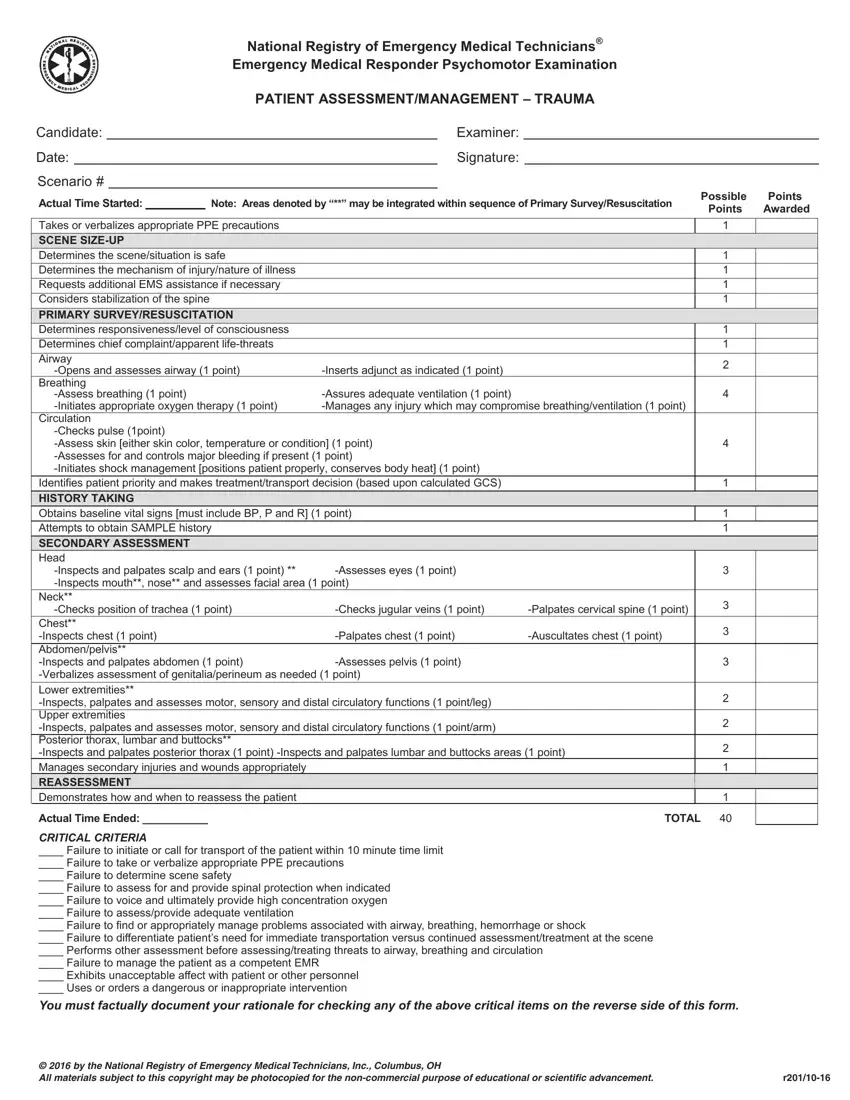
The EMT Trauma Assessment Form serves as a comprehensive guideline and checklist for Emergency Medical Responders (EMRs) during the critical initial assessment and management of trauma patients. Created by the National Registry of Emergency Medical Technicians®, it outlines a structured approach for evaluating the severity and scope of a patient's injuries in a trauma scenario. Beginning with preliminary safety and precautionary measures, the form ensures that responders take or verbalize proper personal protective equipment precautions before sizing up the scene for safety and the mechanism of injury. It further guides the responder through a primary survey/resuscitation phase, focusing on immediate life-threatening conditions through systematic assessment of the airway, breathing, and circulation, including the initiation of appropriate interventions. The form stresses the importance of determining patient priority for treatment and transport based on the Glasgow Coma Scale (GCS). History taking, aimed at gathering baseline vital signs and a SAMPLE history, precedes a thorough secondary assessment, where each part of the body is inspected and assessed for damage or injury. It mandates a reassessment to demonstrate an understanding of when and how to continually reassess the patient. Specific critical criteria detail common pitfalls that could jeopardize patient care, providing a framework for immediate and efficient trauma management. This document not only serves as a guide for EMRs in the field but also as an educational tool to improve the quality of trauma care provided, ensuring that critical steps are not missed and that patients receive the best possible chance at recovery.
| Question | Answer |
|---|---|
| Form Name | Emt Trauma Assessment |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | emt medical assessment scenarios pdf, trauma assessment emt scenarios, nremt emt trauma scenarios, nremt trauma assessment scenarios |
