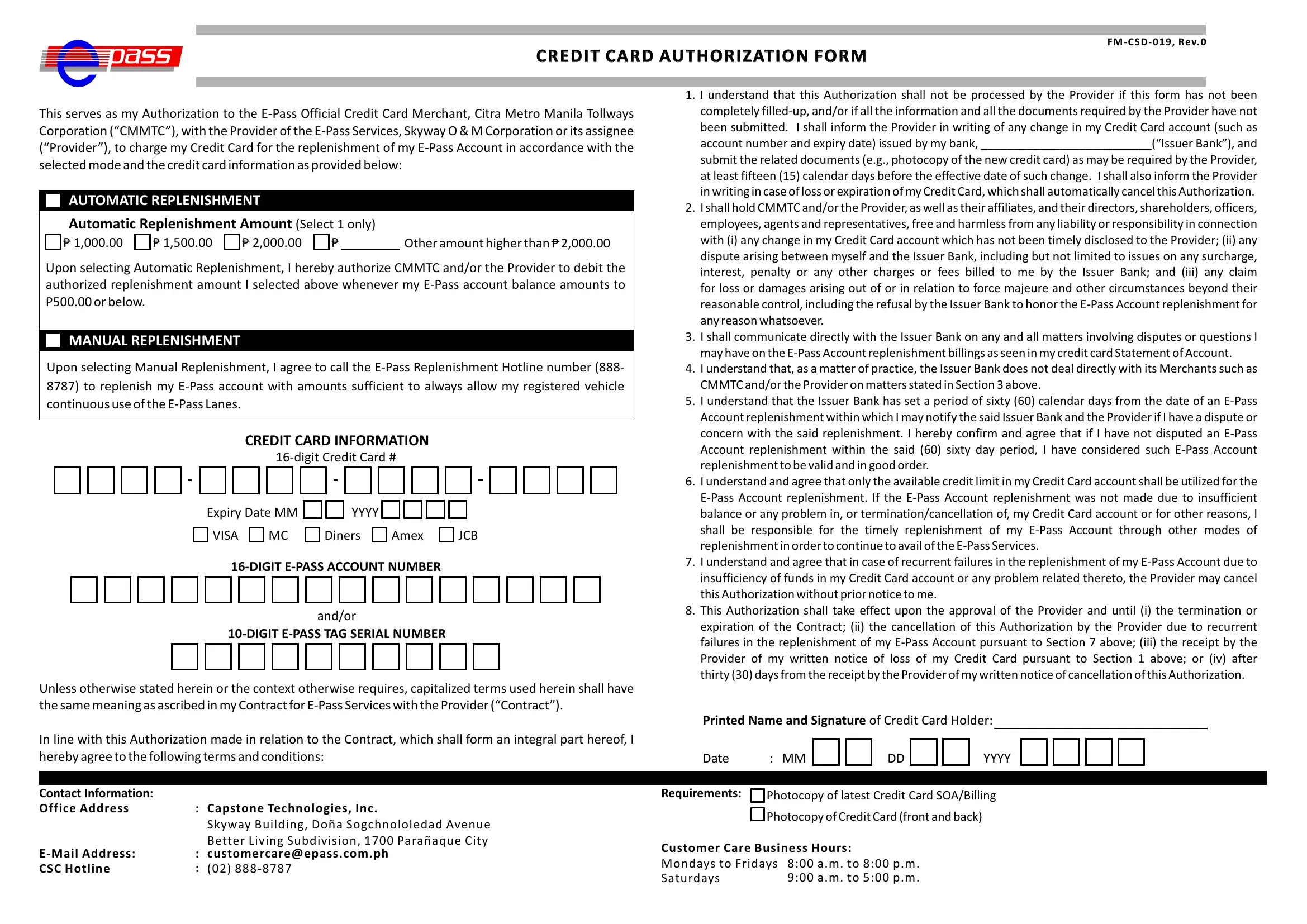
Navigating the landscape of financial transactions has evolved with the advent of electronic payment solutions, amongst which stands the Epass FM CSD 019 form, designed as a credit card authorization template to facilitate seamless toll payments. This particular form embodies an agreement between the credit card holder and the Citra Metro Manila Tollways Corporation (CMMTC) alongside the Skyway O&M Corporation or its assignee, known collectively as the "Provider," aiming to streamline the process of toll collection. By opting into this service, users can choose between automatic or manual replenishment of their E-Pass accounts, ensuring uninterrupted use of the toll lanes. The form meticulously outlines the conditions under which the credit card on file is to be charged for account top-ups, with explicit instructions on how users can manage their accounts, including the requisite steps to address changes to the credit card information, dispute resolution, and the protocol following the loss or expiration of a card. Furthermore, it stresses the importance of timely communication between the cardholder and the issuing bank to mitigate any issues that may arise concerning recharge transactions. Critical too is the understanding that the form's efficacy is contingent upon the accurate and complete submission of information by the user, underlining the mutual responsibilities shared between the toll service provider and the customer to ensure smooth financial transactions. By doing so, it not only epitomizes a commitment to facilitating user convenience but also underscores the evolving nexus between technological advancements and financial management.
| Question | Answer |
|---|---|
| Form Name | Epass Fm Csd 019 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | e pass registration philippines, pass application form, e pass apply online philippines, e pass ph registration |
