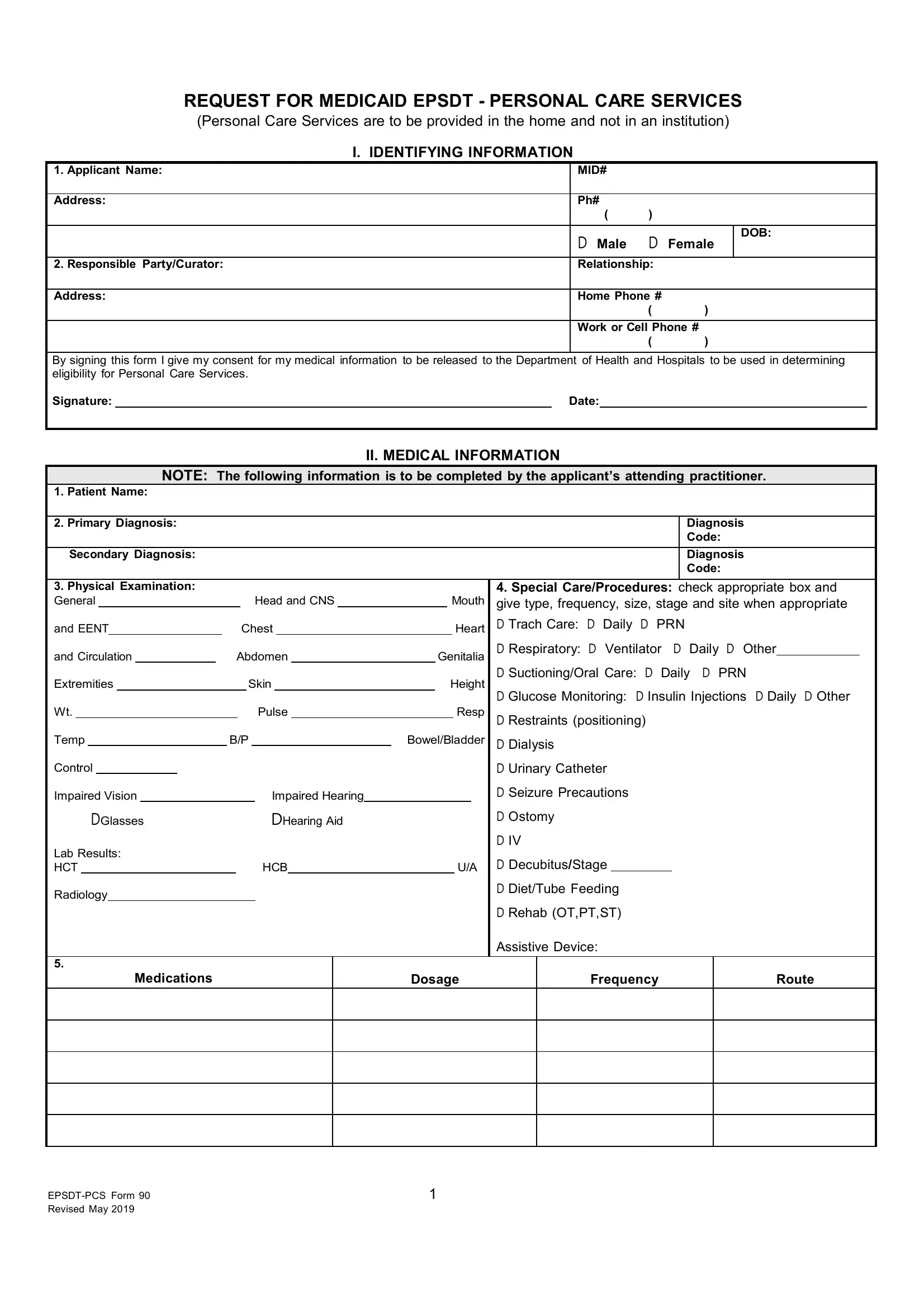
In navigating the complexities of healthcare, one critical document stands out for families requiring in-home personal care services under Medicaid's Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) program: the EPSDT PCS 90 form. This form is a cornerstone in accessing personalized care needed by individuals, enabling them to receive assistance within the comfort of their homes rather than institutional settings. It encompasses several key sections, starting with identifying information which includes the applicant's name, contact details, and important consent for the release of medical information. The crux of the form lies in its detailed medical information section, meticulously filled out by the attending practitioner. This section captures the patient's diagnoses, physical examination findings, details on special care or procedures required, medications, and any recent hospitalizations or mental status evaluations. Furthermore, it assesses the level of care determination, guiding the healthcare provider to evaluate the patient's abilities in performing activities of daily living (ADLs) and determining the need for assistance, ranging from independent to maximal assistance. It even considers whether the patient requires help with mobility or attending medical appointments. Finally, it culminates with the practitioner's order, documenting the necessity and specifics of the prescribed personal care services. This form represents a comprehensive tool designed to ensure patients obtain the level of care they require, marking a crucial step in fostering their health and well-being in a home setting.
| Question | Answer |
|---|---|
| Form Name | Epsdt Pcs 90 Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | epsdt pcs, epsdt forms pdf, epsdt forms for mt, louisiana epsdt form 90 |
REQUEST FOR MEDICAID EPSDT - PERSONAL CARE SERVICES
(Personal Care Services are to be provided in the home and not in an institution)
I. IDENTIFYING INFORMATION
1. Applicant Name: |
MID# |
|
|
|
|
|
|
|
|
Address: |
Ph# |
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
D Male |
D Female |
DOB: |
|
|
|
|||
|
|
|
|
|
2. Responsible Party/Curator: |
Relationship: |
|
|
|
|
|
|
|
|
Address: |
Home Phone # |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
Work or Cell Phone # |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
By signing this form I give my consent for my medical information to be released to the Department of Health and Hospitals to be used in determining eligibility for Personal Care Services.
Signature:Date:
II. MEDICAL INFORMATION
NOTE: The following information is to be completed by the applicant’s attending practitioner.
1. Patient Name:
2. Primary Diagnosis: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diagnosis |
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Secondary Diagnosis: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diagnosis |
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Code: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
3. Physical Examination: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. Special Care/Procedures: check appropriate box and |
||||||||||||||||||||
General |
|
|
|
|
|
|
|
|
|
|
|
|
|
Head and CNS |
|
|
|
|
Mouth |
give type, frequency, size, stage and site when appropriate |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
and EENT |
|
|
|
|
Chest |
|
|
|
|
Heart |
D Trach Care: D Daily |
D PRN |
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D Respiratory: D Ventilator D Daily D Other |
|
|
|||||||||||
and Circulation |
|
|
|
|
Abdomen |
|
|
Genitalia |
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
||||||||||||||||||||||||||||||||||||||
Extremities |
|
|
|
|
|
Skin |
|
|
Height |
D Suctioning/Oral Care: D Daily D PRN |
|
|
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D Glucose Monitoring: |
D Insulin Injections |
D Daily D Other |
|||||||
Wt. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Pulse |
|
|
|
|
|
|
|
Resp |
D Restraints (positioning) |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
Temp |
|
|
|
|
|
|
B/P |
|
|
|
|
Bowel/Bladder |
D Dialysis |
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
Control |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D Urinary Catheter |
|
|
|
|
|
|
|
|||||||||
Impaired Vision |
|
|
|
|
|
|
|
Impaired Hearing |
|
|
|
|
|
|
D Seizure Precautions |
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D Ostomy |
|
|
|
|
|
|
|
||||||||||||
|
|
|
DGlasses |
|
|
|
|
|
|
DHearing Aid |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D IV |
|
|
|
|
|
|
|
||
Lab Results: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D Decubitus/Stage |
|
|
|
|
|
|
|
|
||||||||||||
HCT |
|
|
|
|
|
|
HCB |
|
|
|
|
U/A |
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D Diet/Tube Feeding |
|
|
|
|
|
|
|
||
Radiology |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D Rehab (OT,PT,ST) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Assistive Device: |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dosage |
|
Frequency |
|
Route |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Revised May 2019 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
II. MEDICAL INFORMATION (Continued)
6.Recent Hospitalizations: (include psychiatric):
7.Mental Status/Behavior: Check Yes or No. If Yes, indicate frequency: 1 = seldom; 2 = frequent; 3 = always
Oriented |
D Yes ( 1 |
2 |
3 ) |
D No |
Depressed |
D Yes ( 1 |
2 |
3 |
) |
D No |
Cooperative |
D Yes ( 1 |
2 |
3 |
) |
D No |
|
|
|
|
|
|
Physically |
D Yes ( 1 |
2 |
3 ) |
|
D No |
Verbally |
D Yes ( 1 |
2 |
3 |
) |
D No |
|
Passive |
D Yes ( 1 |
2 |
3 ) |
D No |
Abusive |
|
Abusive |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||
Verbal |
D Yes ( 1 |
2 |
3 ) |
D No |
Comatose |
D Yes |
( 1 |
2 |
3 |
) |
D No |
Hostile |
D Yes ( 1 |
2 |
3 |
) |
D No |
Forgetful |
D Yes ( 1 |
2 |
3 ) |
D No |
Confused |
D Yes |
( 1 |
2 |
3 |
) |
D No |
Combative |
D Yes ( 1 |
2 |
3 |
) |
D No |
Non- |
D Yes ( 1 |
2 |
3 ) |
D No |
Injures |
D Yes ( 1 |
2 |
3 ) |
D No |
|
|
|
|
|
|
||
responsive |
Self/Others |
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
8.Impairments: Please rate the following. 1- Mild ,
Walking |
( 1 |
2 |
3 ) |
Chronic |
( 1 |
2 |
3 |
) |
Vision |
( 1 |
2 |
3 |
) |
|
heart failure |
impairment |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
Spasticity |
( 1 |
2 |
3 ) |
Speech |
( 1 |
2 |
3 |
) |
Oral feeding |
( 1 |
2 |
3 |
) |
|
impairment |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Limb |
|
|
|
Seizure |
|
|
|
|
Bladder and |
|
|
|
|
|
( 1 |
2 |
3 ) |
( 1 |
2 |
3 |
) |
bowel |
( 1 |
2 |
3 |
) |
|||
weakness |
Disorder |
|||||||||||||
|
|
|
|
|
|
|
incontinence |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
Hypotonia |
( 1 |
2 |
3 ) |
Developmental |
( 1 |
2 |
3 |
) |
Intellectual |
( 1 |
2 |
3 |
) |
|
delay |
impairment |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
Chronic |
|
|
|
Hearing |
|
|
|
|
|
|
|
|
|
|
Resp |
( 1 |
2 |
3 ) |
(1 |
2 |
3 ) |
|
|
|
|
|
|||
impairment |
|
|
|
|
|
|||||||||
distress |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
III. LEVEL OF CARE DETERMINATION |
|
|
|
|
||||||
Activities of Daily Living: |
|
|
|
|
|
|
|
|
|
|
||||
Based on |
the beneficiary’s impairment, the attending |
practitioner should |
check the |
appropriate |
box as it applies to |
|||||||||
the beneficiary’s ability to perform this age appropriate tasks using the following definitions and PCS Level of Assistance Guide:
Not Independent at this Age – not age appropriate to perform this task independently Independent – beneficiary able to perform task without assistance
Limited Assistance – beneficiary aids in task, but receives help from other persons some of the time
Extensive Assistance – beneficiary aids in task, but receives help from other persons all of the time Maximal Assistance – beneficiary is entirely dependent on other persons
Note: An additional 15 minutes can be added to bathing, dressing and toileting if mobility/transfer assistance is required
(EPSDT – PCS Level of Assistance Guide)
This is a general guide to assist practitioners with determining the level of assistance beneficiaries require to complete their activities of daily living (ADL). Additional time to complete the tasks will be considered if there is sufficient medical documentation provided. Please use the comments section below and attach documentation to support the need for additional time to complete the ADL’s. In addition to the PCS tasks listed, assistance with incidental household chores may be approved. This does not include routine household chores such as regular laundry, ironing, mopping, dusting, etc., but instead arises as the result of providing assistance with personal care to the beneficiary.
|
|
Levels of Assistance |
|
|
|
PCS Task |
|
|
|
|
Mobility/Transfer Requirement |
|
Independent |
Limited |
Extensive |
Maximal |
|
|
Assistance |
Assistance |
Assistance |
|
|
|
|
|
|||
Bathing |
0 |
15 min |
30 min |
45 min |
Additional 15 min |
|
|
|
|
|
|
Dressing |
0 |
15 min |
30 min |
45 min |
Additional 15 min |
|
|
|
|
|
|
Grooming |
0 |
15 min |
15 min |
15 min |
|
|
|
|
|
|
|
Toileting |
0 |
15 min |
30 min |
45 min |
Additional 15 min |
|
|
|
|
|
|
Eating |
0 |
15 min |
30 min |
45 min |
|
Meal Prep |
0 |
30 min |
30 min |
30 min |
|
|
|
|
|
|
|
2
Revised May 2019
III. LEVEL OF CARE DETERMINATION (Continued)
NOTE: The following information is to be completed by the applicant’s attending practitioner. Check the appropriate box using the definitions and EPSDT PCS Level of Assistance Guide to assist with determining the level of care.
|
|
|
|
Not |
|
|
Limited |
Extensive |
|
Maximal |
|
|
|
|
|
||
|
|
Activity |
|
Independent |
Independent |
|
|
|
Comments |
|
|||||||
|
|
|
|
Assistance |
Assistance |
Assistance |
|
|
|||||||||
|
|
|
|
at this Age |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Bathing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dressing |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Grooming |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Toileting |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Eating |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Level of care is provided under classifications dependent upon the type and/or complexity of care and services rendered, as well as, the |
|
||||||||||||||
|
|
amount of time required to render the necessary care and services. Please select one of the following: |
|
|
|
|
|||||||||||
|
|
This individual’s condition includes a need for nursing care to manage a plan of care and/or more assistance with extensive personal care, |
|
||||||||||||||
|
|
ambulation, and mobilization. May include professional nursing care and assessment on a daily basis due to a serious condition which is |
|
||||||||||||||
|
|
unstable or a rehabilitative therapeutic regime requiring professional staff. |
|
|
|
|
|||||||||||
|
|
D Yes, this individual requires this level of care. |
|
|
|
|
|
|
|
|
|||||||
|
|
D No, this individual does not require this level of care. |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
Mobility/Transfer Requirements: Please indicate below the activities of daily living for which the beneficiary will require assistance with |
|
||||||||||||||
|
|
mobility/transfer. |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Bathing |
D Yes D No |
Dressing D Yes D No |
Toileting |
D Yes D No |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical Appointments: |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Will the beneficiary need the PCS worker to accompany him/her to medical appointments? D Yes D No |
|
|
|
|
|||||||||||
|
|
How often will the beneficiary have scheduled medical appointments? |
D weekly D monthly D quarterly D other |
|
|||||||||||||
|
|
Reason for PCS worker to accompany child to medical appointments: |
|
|
|
|
|
|
|
||||||||
IV. PRACTITIONER’S ORDER |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
The above named patient is in need of EPSDT PCS due to his/her current medical condition. I am prescribing |
|
|
|||||||||||||
|
|
Personal Care Services for |
|
hours, |
|
days a week as determined by the level of care determination. |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Practitioner’s Name (type or print):
Address:
Phone:
()
I certify/recertify that I am the attending practitioner for this patient and that the information provided is accurate and correct to the best of my knowledge. I authorize these EPSDT personal care services and will periodically review the plan. In my professional opinion, the services listed on this form are medically necessary and appropriate due to the child’s medical condition. I understand that if I knowingly authorize services that are not medically necessary, I may be in violation of Medicaid rules and subject to sanctions described therein. I understand a face to face evaluation must be held between beneficiary and practitioner.
Practitioner’s Signature |
|
Date |
3
Revised May 2019
4
Revised May 2019