
Using PDF forms online is a piece of cake with this PDF tool. You can fill in 90l form printable here painlessly. The tool is consistently improved by our staff, getting new awesome functions and growing to be even more versatile. Starting is effortless! Everything you should do is adhere to these easy steps below:
Step 1: Click on the "Get Form" button above on this webpage to open our editor.
Step 2: With this online PDF tool, you'll be able to do more than just fill out forms. Try all of the features and make your forms seem sublime with customized textual content added, or adjust the original input to excellence - all that comes along with an ability to add any photos and sign the PDF off.
This PDF doc will involve specific details; to ensure accuracy, you need to pay attention to the following suggestions:
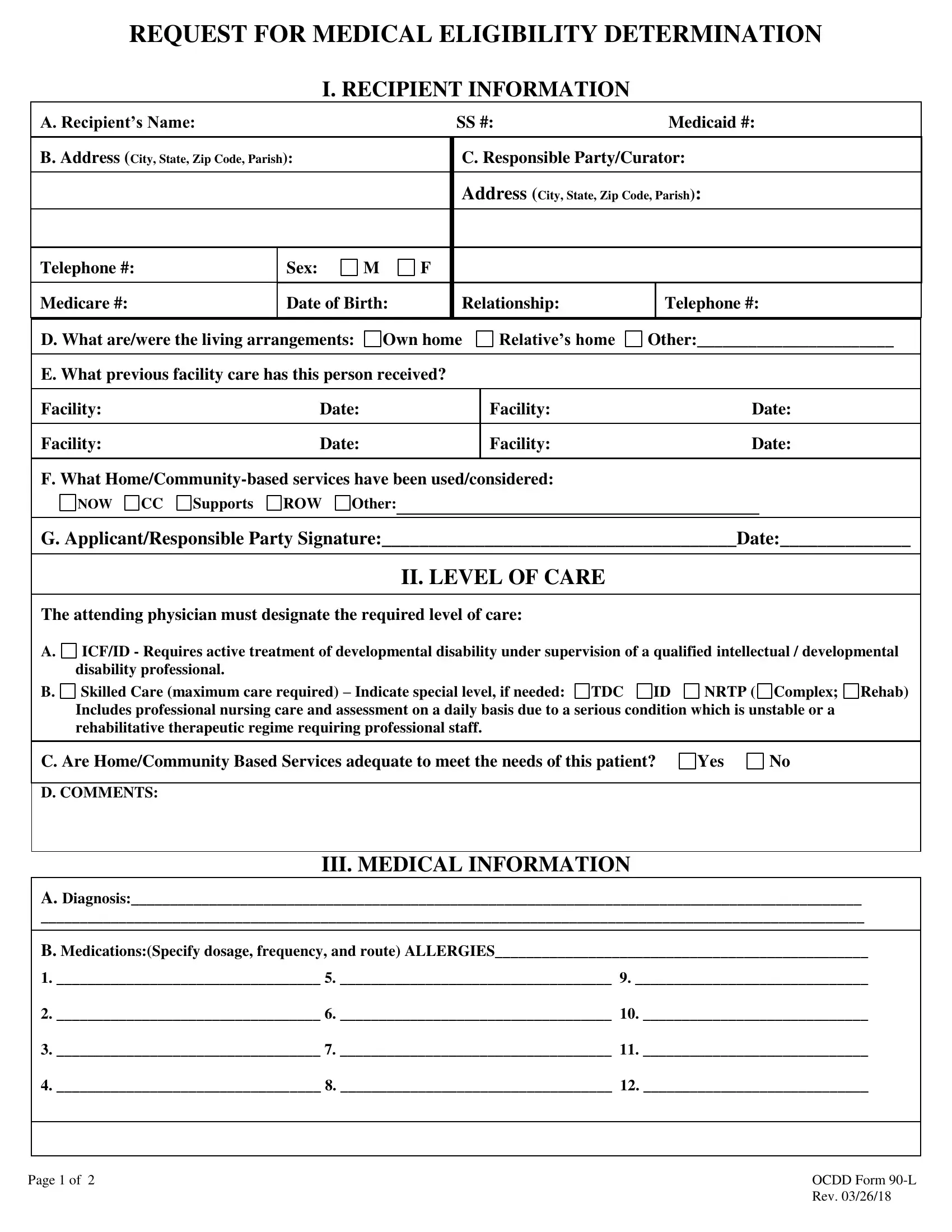
1. For starters, while filling out the 90l form printable, beging with the part that has the subsequent fields:
2. Given that this part is finished, you should put in the essential specifics in A Recipients Name SS B Address, Supports ROW Other, NOW CC G ApplicantResponsible, II LEVEL OF CARE, The attending physician must, ICFID Requires active treatment, NRTP Complex Rehab, C Are HomeCommunity Based Services, D COMMENTS, III MEDICAL INFORMATION, and A Diagnosis B MedicationsSpecify allowing you to proceed to the third part.
3. This next segment is considered pretty uncomplicated, Page of, and OCDD Form L Rev - all these blanks needs to be filled out here.
4. The next part needs your input in the subsequent parts: Recipients Name, C Recent Hospitalizations D, Yes No Oriented Yes No, Yes No Comatose Yes No, Yes No Hostile Yes No, E Communications Verbal Nonverbal, Eating Bathing Personal, Impaired vision, Glasses, Impaired hearing, Hearing Aid, Dentures, and G SPECIAL CAREPROCEDURES check. Be sure to fill in all required info to go forward.
Always be really careful while filling out C Recent Hospitalizations D and Recipients Name, as this is the section where many people make a few mistakes.
5. Last of all, this last subsection is what you'll have to wrap up prior to finalizing the PDF. The fields at this point include the next: Ostomy care Glucose Monitoring, DietTube Feeding Dialysis, Ventilator Dependent Other, and H PHYSICAL EXAMINATION.
Step 3: Immediately after going through your fields and details, press "Done" and you're done and dusted! Right after starting a7-day free trial account with us, you will be able to download 90l form printable or send it via email directly. The file will also be easily accessible from your personal account page with your every single modification. FormsPal is committed to the privacy of all our users; we always make sure that all personal information coming through our system is confidential.