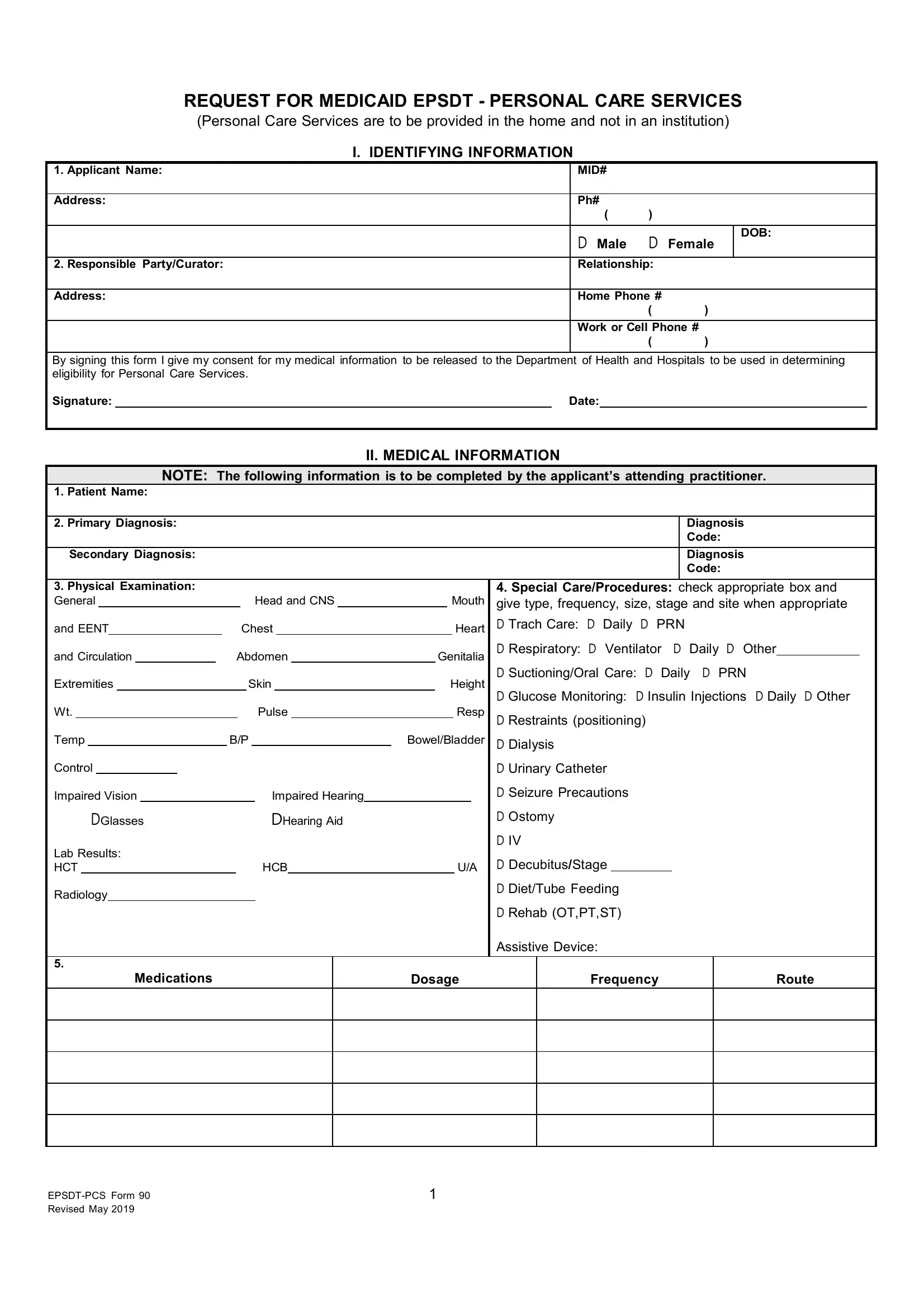
In navigating the complexities of healthcare, one critical document stands out for families requiring in-home personal care services under Medicaid's Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) program: the EPSDT PCS 90 form. This form is a cornerstone in accessing personalized care needed by individuals, enabling them to receive assistance within the comfort of their homes rather than institutional settings. It encompasses several key sections, starting with identifying information which includes the applicant's name, contact details, and important consent for the release of medical information. The crux of the form lies in its detailed medical information section, meticulously filled out by the attending practitioner. This section captures the patient's diagnoses, physical examination findings, details on special care or procedures required, medications, and any recent hospitalizations or mental status evaluations. Furthermore, it assesses the level of care determination, guiding the healthcare provider to evaluate the patient's abilities in performing activities of daily living (ADLs) and determining the need for assistance, ranging from independent to maximal assistance. It even considers whether the patient requires help with mobility or attending medical appointments. Finally, it culminates with the practitioner's order, documenting the necessity and specifics of the prescribed personal care services. This form represents a comprehensive tool designed to ensure patients obtain the level of care they require, marking a crucial step in fostering their health and well-being in a home setting.
| Question | Answer |
|---|---|
| Form Name | Epsdt Pcs 90 Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | epsdt pcs, epsdt forms pdf, epsdt forms for mt, louisiana epsdt form 90 |
