Eta Form 9062 is a U.S. Citizenship and Immigration Services form that is used to apply for various benefits associated with being a lawful permanent resident of the United States. The form can be used to apply for a Permanent Resident Card (commonly known as a "green card"), change or correct your name on your green card, request an extension of stay or change of status, and file Form I-539, Application to Extend/Change Nonimmigrant Status. The Eta Form 9062 application process can be complex, so it is important to understand the specific requirements associated with each benefit you are applying for. For more information on how to complete the Eta Form 9062 application process, please visit the U.S. Citizenship and Immigration Services website.
| Question | Answer |
|---|---|
| Form Name | Eta Form 9062 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | form 9062, 2006, CN, form 9062 pdf |
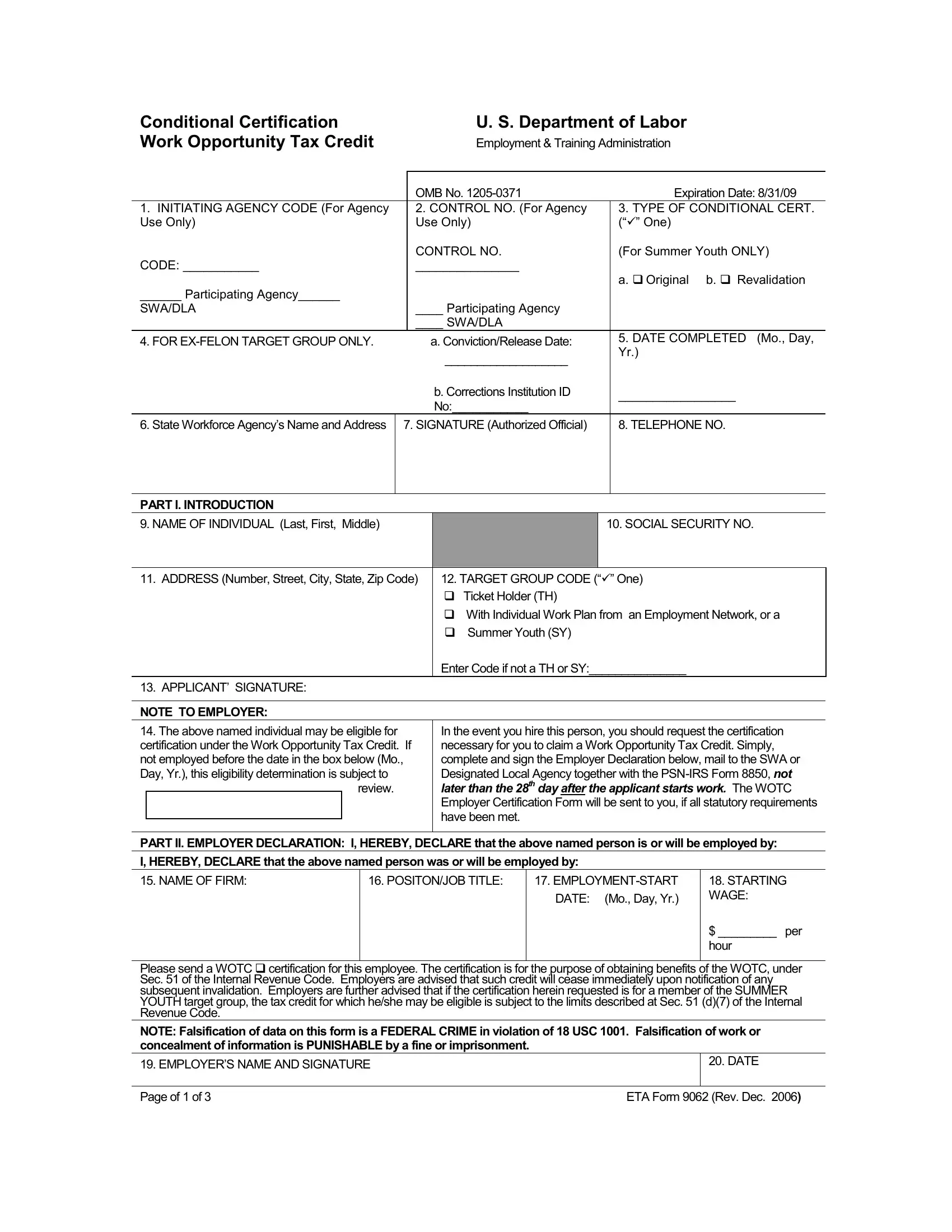
Conditional Certification |
|
|
U. S. Department of Labor |
|||
Work Opportunity Tax Credit |
|
|
Employment & Training Administration |
|||
|
|
|
|
|
|
|
|
|
OMB No. |
|
Expiration Date: 8/31/09 |
||
1. INITIATING AGENCY CODE (For Agency |
|
2. CONTROL NO. (For Agency |
|
3. TYPE OF CONDITIONAL CERT. |
||
Use Only) |
|
Use Only) |
|
(“” One) |
||
|
|
CONTROL NO. |
|
(For Summer Youth ONLY) |
||
CODE: ___________ |
|
_______________ |
|
|
|
|
|
|
|
|
|
|
a. Original b. Revalidation |
______ Participating Agency______ |
|
|
|
|
|
|
SWA/DLA |
|
____ Participating Agency |
|
|
||
|
|
____ SWA/DLA |
|
|
||
4. FOR |
|
a. Conviction/Release Date: |
|
5. DATE COMPLETED (Mo., Day, |
||
|
|
Yr.) |
||||
|
___________________ |
|
|
|||
|
|
|
|
|||
|
|
|
b. Corrections Institution ID |
|
_________________ |
|
|
|
|
No:___________ |
|
|
|
6. State Workforce Agency’s Name and Address |
7. SIGNATURE (Authorized Official) |
|
8. TELEPHONE NO. |
|||
|
|
|
|
|
|
|
PART I. INTRODUCTION |
|
|
|
|
|
|
9. NAME OF INDIVIDUAL (Last, First, Middle) |
|
|
|
|
10. SOCIAL SECURITY NO. |
|
|
|
|
|
|
|
|
11. ADDRESS (Number, Street, City, State, Zip Code) 12. TARGET GROUP CODE (“” One) |
||||||
Ticket Holder (TH)
With Individual Work Plan from an Employment Network, or a
Summer Youth (SY)
|
|
|
Enter Code if not a TH or SY:_______________ |
13. APPLICANT’ SIGNATURE: |
|
||
|
|
|
|
NOTE TO EMPLOYER: |
|
||
14. The above named individual may be eligible for |
In the event you hire this person, you should request the certification |
||
certification under the Work Opportunity Tax Credit. If |
necessary for you to claim a Work Opportunity Tax Credit. Simply, |
||
not employed before the date in the box below (Mo., |
complete and sign the Employer Declaration below, mail to the SWA or |
||
Day, Yr.), this eligibility determination is subject to |
Designated Local Agency together with the |
||
|
|
review. |
later than the 28th day after the applicant starts work. The WOTC |
|
|
|
Employer Certification Form will be sent to you, if all statutory requirements |
|
|
|
have been met. |
|
|
|
|
|
|
|
|
PART II. EMPLOYER DECLARATION: I, HEREBY, DECLARE that the above named person is or will be employed by:
I, HEREBY, DECLARE that the above named person was or will be employed by:
15. NAME OF FIRM: |
16. POSITON/JOB TITLE: |
17. |
18. STARTING |
|
|
DATE: (Mo., Day, Yr.) |
WAGE: |
|
|
|
|
|
|
|
$ _________ per |
|
|
|
hour |
|
|
|
|
Please send a WOTC certification for this employee. The certification is for the purpose of obtaining benefits of the WOTC, under Sec. 51 of the Internal Revenue Code. Employers are advised that such credit will cease immediately upon notification of any subsequent invalidation. Employers are further advised that if the certification herein requested is for a member of the SUMMER YOUTH target group, the tax credit for which he/she may be eligible is subject to the limits described at Sec. 51 (d)(7) of the Internal Revenue Code.
NOTE: Falsification of data on this form is a FEDERAL CRIME in violation of 18 USC 1001. Falsification of work or concealment of information is PUNISHABLE by a fine or imprisonment.
19. EMPLOYER’S NAME AND SIGNATURE
20. DATE
Page of 1 of 3 |
ETA Form 9062 (Rev. Dec. 2006) |

CONDITIONAL CERTIFICATION (CC) ETA FORM 9062. When a SWA/DLA or Participating Agency (PA) determines that a job- ready applicant is, tentatively, ELIGIBLE as a member of a target group for the consolidated WOTC, it shall use this required form, without modification, to show that an eligibility determination was made for this person. Note. The CC serves as an official record of the
INSTRUCTIONS FOR COMPLETING THE “CONDITIONAL CERTIFICATION” FORM. (Boxes
Box 1: |
Initiating Agency Code. If the CC was issued by a participating agency (PA), enter its code. SWAs/DLAs assign codes |
|
to designate each PA and indicate the initiating source for the eligibility determination process. If the eligibility |
|
determination was performed by the SWA/DLA, enter the SWA/DLA code, if available. Indicate with a check mark “” if |
|
initiating agency is aParticipatingAgency or SWA/DLA. |
Box 2: |
Control Number. Usually the PA determines thecontrol number (CN). However, SWAs/DLAs may, for internal control |
|
purposes, develop their own CNsystem. It may be aSocial Security No., case no., or some other appropriate designation, which |
|
permits easy filing, certification and retrieval of forms. Enter corresponding CN and indicate with a check mark “” whether the |
|
source is aPA or a SWA/DLA. |
Box 3: |
Type of Conditional Certification. This system distinguishes between “Original,” if the individual is being processed for thefirst |
|
time, or “Revalidation,” if the eligibility process was performed within the previous |
|
Youth target group only). Otherwise, the Conditional Certification is counted as “Original.” Indicate with a check mark “” whether |
|
eligibility determination is “Original” or “Revalidation.” |
Box 4: |
For |
|
verifyingtarget group eligibility. |
Box 5: |
Date Completed. Enter themonth, day, year in which the eligibility determination was completed. |
Box 6: |
SWA/DLAName and Address. (If known, enter orstamp the name and address, including zipcode, of theSWA/DLA |
|
responsible for Certifications requests for the employer indicated in Box 16. Leave blank if SWA/DLA’s name and address is |
|
unknown. |
Box 7: |
Signature. Entersignature of the authorized |
Box 8: |
Telephone No. Enter corresponding SWA/DLA or participating agency area code, telephone number and extension, if available. |
PART I. |
INTRODUCTION: |
Box 9: |
Name of Individual. Enter the individual’s/applicant’s full name (i.e., last name, first name and middle initial). |
Box 10: |
Social SecurityNumber. Enterthe individual’s/applicant social security number. |
Box 11: |
Address/Telephone No. Enter the individual’s/applicant’s home address, including apartment number and zip code. After |
|
address, enter individual’s/applicant’s telephone number, including area code. |
Box 12: |
Target Group Code. Enter acheck mark “” to indicate if “SummerYouth, “Ticket Holder (TH)” with an IWP from an |
|
Employment Network (EN) or Other.” If different from SummerYouth or Ticket Holder, enter codefor specificWOTC target |
|
group based on client’s information and documentation provided. |
Box 13: |
Signature. Get Individual’s/applicant’s signature. If aminor, parent or guardianmust sign here. |
Box 14: |
CC ValidityPeriod. (This box is to becompleted by the SWA/DLA or PA). Enter the month/day/year when the CC expires |
|
(e.g. 45 days for Summer Youth) |
Page 2 of 3 |
ETA Form 9062 (Rev. Dec. 2006) |
PART II. EMPLOYER DECLARATION:
Box 15: Name of Firm. Enter full name of the employing firm (the firm where the employee will actually work).
Box 16: Position/Job Title. Enter the position or jobtitle the employee will hold.
Box 17:
Box 18: Starting Wage. Enter the wage or salary which the employee will be paid. If not known, enter an estimated wage.
Box 19: Employer’s Name and Signature. Enter employer’s corresponding signature here.
Box 20. Date. Enter month, day and year when you signed this form.
Persons are not required to respond to this collection of information unless it displays a currently valid OMB Control Number. Respondents’ obligation to reply to these requirements for obtaining the tax credit per P.L.
Page 3 of 3 |
ETA 9062 (Rev. Dec. 2006) |