
When you would like to fill out please prescription form blank, it's not necessary to download and install any sort of software - just make use of our PDF editor. To keep our editor on the forefront of practicality, we aim to put into practice user-oriented capabilities and improvements on a regular basis. We are at all times looking for suggestions - assist us with reshaping how we work with PDF docs. Here is what you would want to do to start:
Step 1: Simply click on the "Get Form Button" above on this site to access our pdf form editor. Here you will find all that is necessary to fill out your file.
Step 2: As soon as you access the editor, you will notice the document all set to be completed. Apart from filling in various blanks, you might also do some other things with the PDF, including writing custom textual content, editing the original textual content, adding images, affixing your signature to the PDF, and much more.
To be able to finalize this document, ensure that you enter the right information in every field:
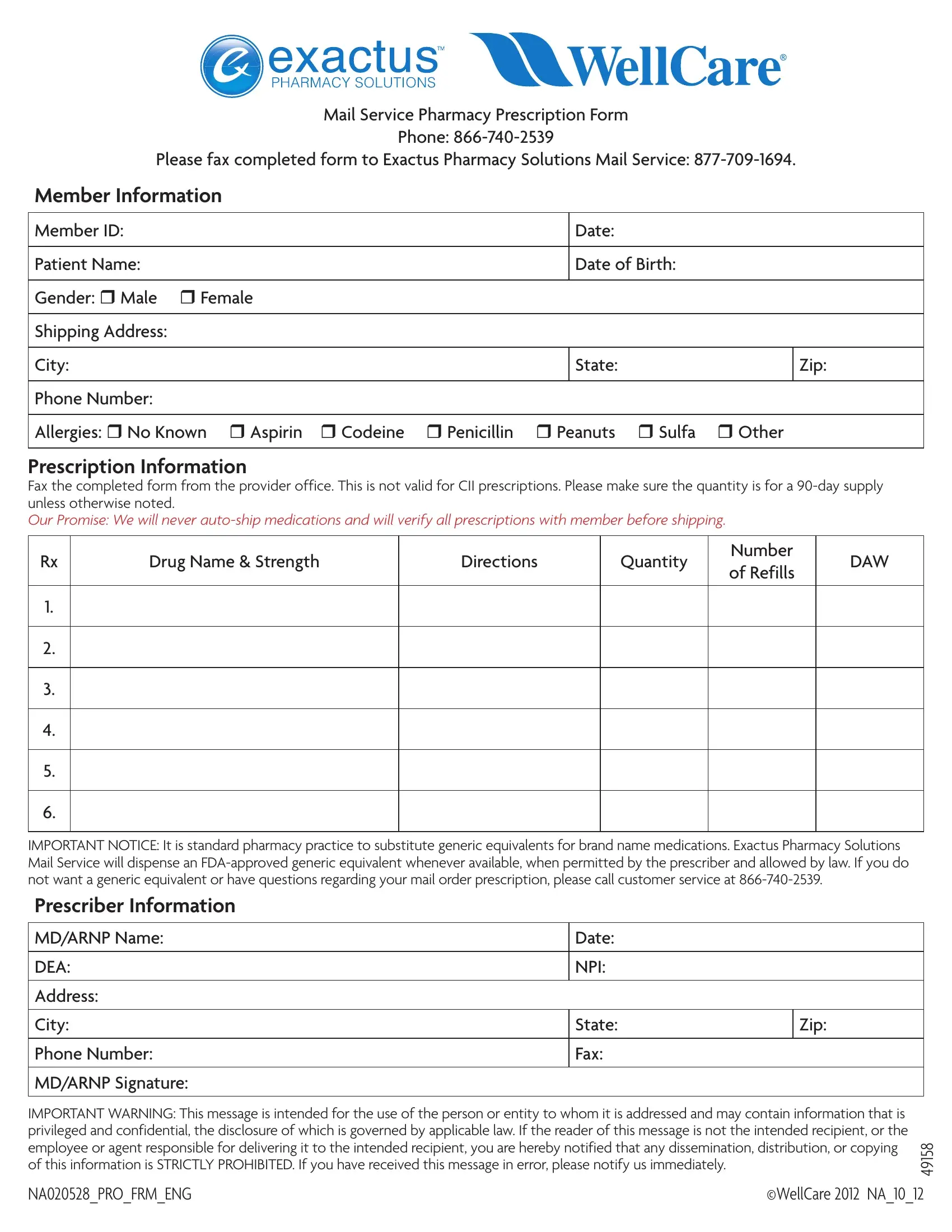
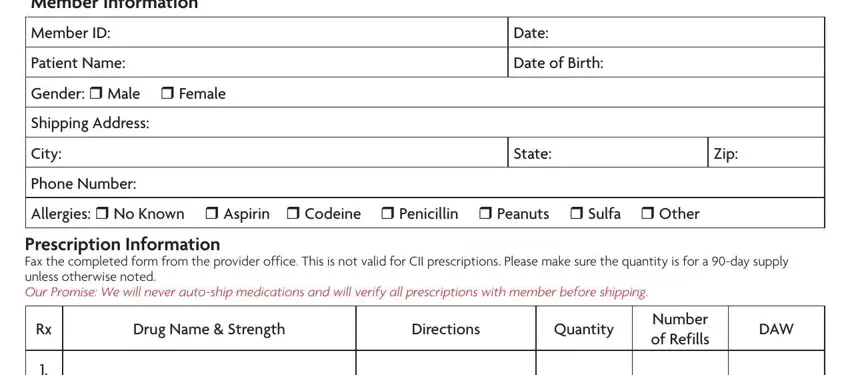
1. It's very important to complete the please prescription form blank accurately, hence be attentive when filling out the parts comprising all of these blank fields:
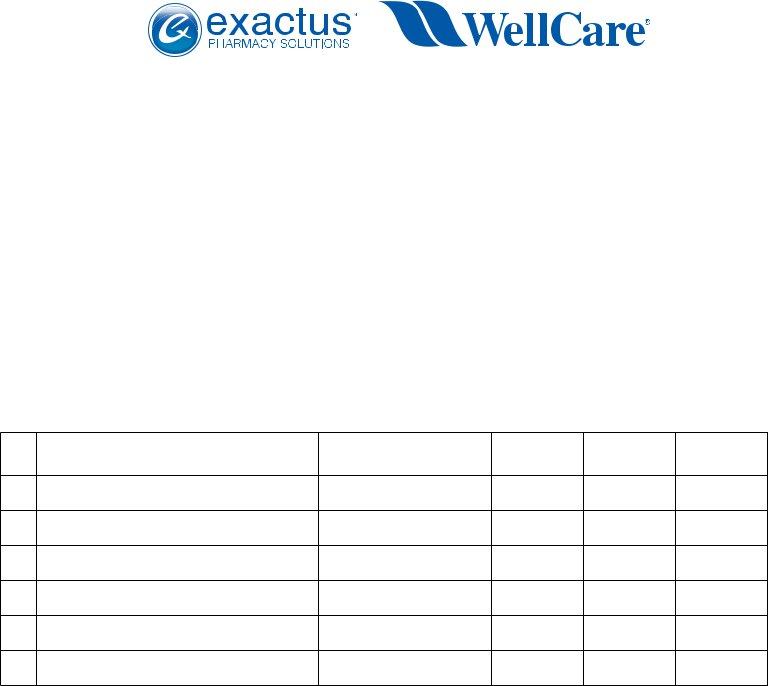
2. When this section is filled out, go to type in the relevant details in all these: IMPORTANT NOTICE It is standard, MDARNP Name, DEA, Address, City, Phone Number, MDARNP Signature, Date, NPI, State, Fax, and Zip.

People who work with this document often make mistakes when filling out IMPORTANT NOTICE It is standard in this area. Be sure you revise whatever you type in right here.
Step 3: Revise everything you've inserted in the blanks and click on the "Done" button. Make a free trial account with us and acquire immediate access to please prescription form blank - download or modify inside your personal cabinet. FormsPal ensures your data privacy by having a secure method that never saves or distributes any sort of personal information typed in. Rest assured knowing your files are kept protected when you use our editor!