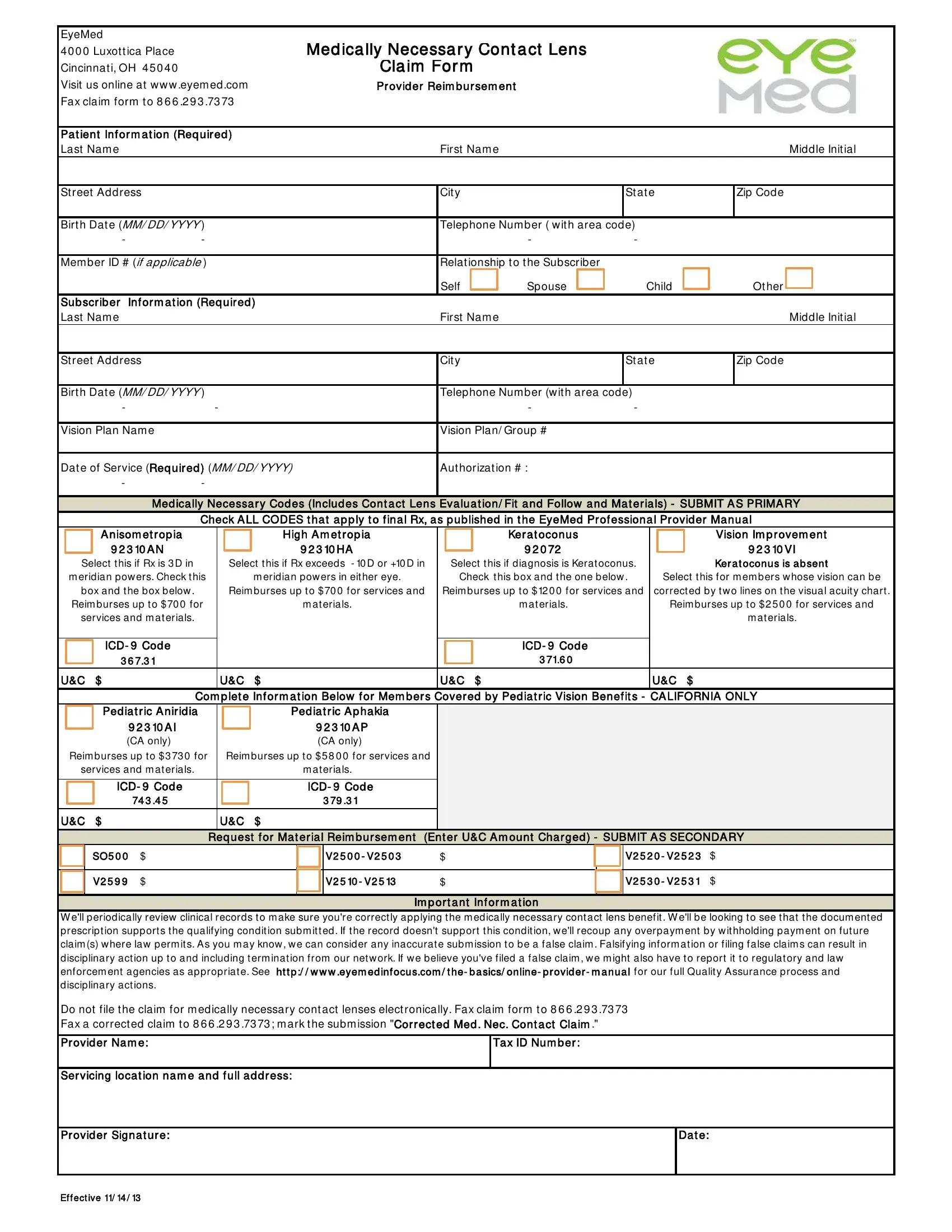
For individuals with specific eye conditions, the accuracy and care in selecting the correct contact lenses are not just a matter of comfort, but a necessity. The EyeMed Medically Necessary Contact Lens Claim Form serves as a critical tool in ensuring these patients receive the medically necessary contact lenses prescribed by their eye care professionals. Centrally located at the Luxottica Place in Cincinnati, OH, this form is designed for eye care providers to claim reimbursement for services rendered and materials provided to patients under specific medical conditions such as Anisometropia, High Ametropia, and Keratoconus, among others. The form outlines detailed patient and subscriber information, the required medical necessity codes that justify the use of such lenses, and the associated reimbursement caps for these services and materials. Additionally, it contains specific sections for pediatric patients within California, reflecting unique requirements for this group. Important information on the submission process highlights the strict adherence to proper documentation and the potential consequences of submitting inaccurate claims, underscoring the importance of precision in every step of the claim process. With the convenient option to fax the completed form, EyeMed simplifies the administrative work for providers while focusing on the broader goal of affording patients the vision correction they medically require.
| Question | Answer |
|---|---|
| Form Name | Eyemed Medically Necessary Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | eyemed medically necessary contacts, eyemed medically online, eyemed lens claim form, pdf80kb form from illinois state pension plan eye med |
|
EyeMed |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
4 0 0 0 Luxot t ica Place |
|
|
|
|
Med ica lly Necessa r y Cont a ct Lens |
|
|
|
|
|
|
|
|
|
||||||||||||
|
Cincinnat i, OH 4 5 0 4 0 |
|
|
|
|
|
|
Cla im For m |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Visit us online at w w w .eyem ed .com |
|
|
|
Pr ovid er Reim b ur sem ent |
|
|
|
|
|
|
|
|
|
|||||||||||||
|
Fax claim form t o 8 6 6 .2 9 3 .73 73 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Pa t ient Inf or m a t ion (Req uir ed ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Last Nam e |
|
|
|
|
|
|
|
|
First Nam e |
|
|
|
|
|
|
|
Middle Init ial |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
St reet Address |
|
|
|
|
|
|
|
Cit y |
|
|
|
|
|
St at e |
|
Zip Code |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Birt h Dat e (MM/ DD/ YYYY ) |
|
|
|
|
|
|
|
Telephone Num ber ( w it h area code) |
|
|
|
|
|
|
|
|
||||||||||
|
- |
- |
|
|
|
|
|
|
|
|
|
- |
|
|
|
- |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mem ber ID # (if applicable ) |
|
|
|
|
|
|
|
Relat ionship t o t he Subscriber |
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
Self |
|
Spouse |
|
|
|
|
Child |
|
|
Ot her |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sub scr ib er Inf or m a t ion (Req uir ed ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Last Nam e |
|
|
|
|
|
|
|
|
First Nam e |
|
|
|
|
|
|
|
Middle Init ial |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
St reet Address |
|
|
|
|
|
|
|
Cit y |
|
|
|
|
|
St at e |
|
Zip Code |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Birt h Dat e (MM/ DD/ YYYY ) |
|
|
|
|
|
|
|
Telephone Num ber (w it h area code) |
|
|
|
|
|
|
|
|
||||||||||
|
- |
|
- |
|
|
|
|
|
|
|
- |
|
|
|
- |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vision Plan Nam e |
|
|
|
|
|
|
|
Vision Plan/ Group # |
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Dat e of Service (Req uir ed ) (MM/ DD/ YYYY) |
Aut horizat ion # : |
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
- |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Med ica lly Necessa r y Cod es (Includ es Cont a ct Lens Eva lua t ion/ Fit a nd Follow a nd Ma t er ia ls) - SUBMIT A S PRIMA RY |
|||||||||||||||||||||||
|
|
|
|
Check A LL CODES t ha t a p p ly t o f ina l Rx, a s p ub lished in t he EyeMed Pr of essiona l Pr ovid er Ma nua l |
|||||||||||||||||||||||
|
|
|
A nisom et r op ia |
|
|
|
High A m et r op ia |
|
|
|
Ker a t oconus |
|
|
|
|
|
Vision Im p r ovem ent |
||||||||||
|
|
|
9 2 3 10 A N |
|
|
|
|
9 2 3 10 HA |
|
|
9 2 0 72 |
|
|
|
|
|
|
|
|
|
9 2 3 10 VI |
||||||
|
Select t his if Rx is 3 D in |
|
|
Select t his if Rx exceeds - 10 D or +10 D in |
|
Select t his if diagnosis is Kerat oconus. |
|
|
|
|
Ker a t oconus is a b sent |
||||||||||||||||
|
m eridian pow ers. Check t his |
|
|
|
m eridian pow ers in eit her eye. |
|
Check t his box and t he one below . |
|
|
Select t his for m em bers w hose vision can be |
|||||||||||||||||
|
box and t he box below . |
|
|
Reim burses up t o $ 70 0 for services and |
Reim burses up t o $ 12 0 0 for services and |
|
correct ed by t w o lines on t he visual acuit y chart . |
||||||||||||||||||||
|
Reim burses up t o $ 70 0 for |
|
|
|
|
m at erials. |
|
|
|
m at erials. |
|
|
|
Reim burses up t o $ 2 5 0 0 for services and |
|||||||||||||
|
services and m at erials. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
m at erials. |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ICD- 9 Cod e |
|
|
|
|
|
|
|
|
|
|
ICD- 9 Cod e |
|
|
|
|
|
|
|
|
|
||||
|
|
|
3 6 7.3 1 |
|
|
|
|
|
|
|
|
|
3 71.6 0 |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
U&C $ |
|
|
U&C |
$ |
|
|
|
U&C |
$ |
|
|
|
|
|
|
U&C $ |
|
|
|
|
||||||
|
|
|
|
Com p let e Inf or m a t ion Below f or Mem b er s Cover ed b y Ped ia t r ic Vision Benef it s - CA LIFORNIA ONLY |
|||||||||||||||||||||||
|
|
|
Ped ia t r ic A nir id ia |
|
|
|
Ped ia t r ic A p ha kia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
9 2 3 10 A I |
|
|
|
|
9 2 3 10 A P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
(CA only) |
|
|
|
|
(CA only) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Reim burses up t o $ 3 73 0 for |
|
|
Reim burses up t o $ 5 8 0 0 for services and |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
services and m at erials. |
|
|
|
|
m at erials. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
ICD- 9 Cod e |
|
|
|
|
ICD- 9 Cod e |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
74 3 .4 5 |
|
|
|
3 79 .3 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
U&C $ |
|
|
U&C |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
Req uest f or Ma t er ia l Reim b ur sem ent (Ent er U&C A m ount Cha r ged ) - SUBMIT A S SECONDA RY |
||||||||||||||||||||||
|
|
|
SO5 0 0 |
$ |
|
|
|
|
|
|
V2 5 0 0 - V2 5 0 3 |
$ |
|
|
|
|
|
|
V2 5 2 0 - V2 5 2 3 |
$ |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
V2 5 9 9 |
$ |
|
|
|
|
|
|
V2 5 10 - V2 5 13 |
$ |
|
|
|
|
|
|
V2 5 3 0 - V2 5 3 1 |
$ |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Im p or t a nt Inf or m a t ion |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W e'll periodically review clinical records t o m ake sure you're correct ly applying t he m edically necessary cont act lens benefit . W e'll be looking t o see t hat t he docum ent ed prescript ion support s t he qualifying condit ion subm it t ed . If t he record doesn't support t his condit ion, w e'll recoup any overpaym ent by w it hholding paym ent on fut ure claim (s) w here law perm it s. As you m ay know , w e can consider any inaccurat e subm ission t o be a false claim . Falsifying inform at ion or filing false claim s can result in disciplinary act ion up t o and including t erm inat ion from our net w ork. If w e believe you've filed a false claim , w e m ight also have t o report it t o regulat ory and law enforcem ent agencies as appropriat e. See ht t p :/ / w w w .eyem ed inf ocus.com / t he- b a sics/ online- p r ovid er - m a nua l for our full Qualit y Assurance process and disciplinary act ions.
Do not file t he claim for m edically necessary cont act lenses elect ronically. Fax claim form t o 8 6 6 .2 9 3 .73 73
Fax a correct ed claim t o 8 6 6 .2 9 3 .73 73 ; m ark t he subm ission "Cor r ect ed Med . Nec. Cont a ct Cla im ."
Pr ovid er Na m e: |
Ta x ID Num b er : |
|
|
|
|
Ser vicing loca t ion na m e a nd f ull a d d r ess: |
|
|
|
|
|
Pr ovid er Signa t ur e: |
|
Da t e: |
|
|
|
Ef f ect ive 11/ 14 / 13