
Dealing with PDF documents online is very easy using our PDF tool. Anyone can fill out F 82009 Form here without trouble. The tool is continually improved by our staff, acquiring new features and growing to be much more convenient. All it takes is a couple of simple steps:
Step 1: Just click the "Get Form Button" above on this site to launch our pdf form editing tool. Here you will find everything that is required to work with your document.
Step 2: As you start the PDF editor, you will find the form all set to be filled in. Other than filling in various fields, you may as well do other sorts of things with the PDF, particularly adding custom textual content, changing the original text, inserting graphics, affixing your signature to the document, and more.
It is actually straightforward to finish the form adhering to our detailed tutorial! Here is what you have to do:
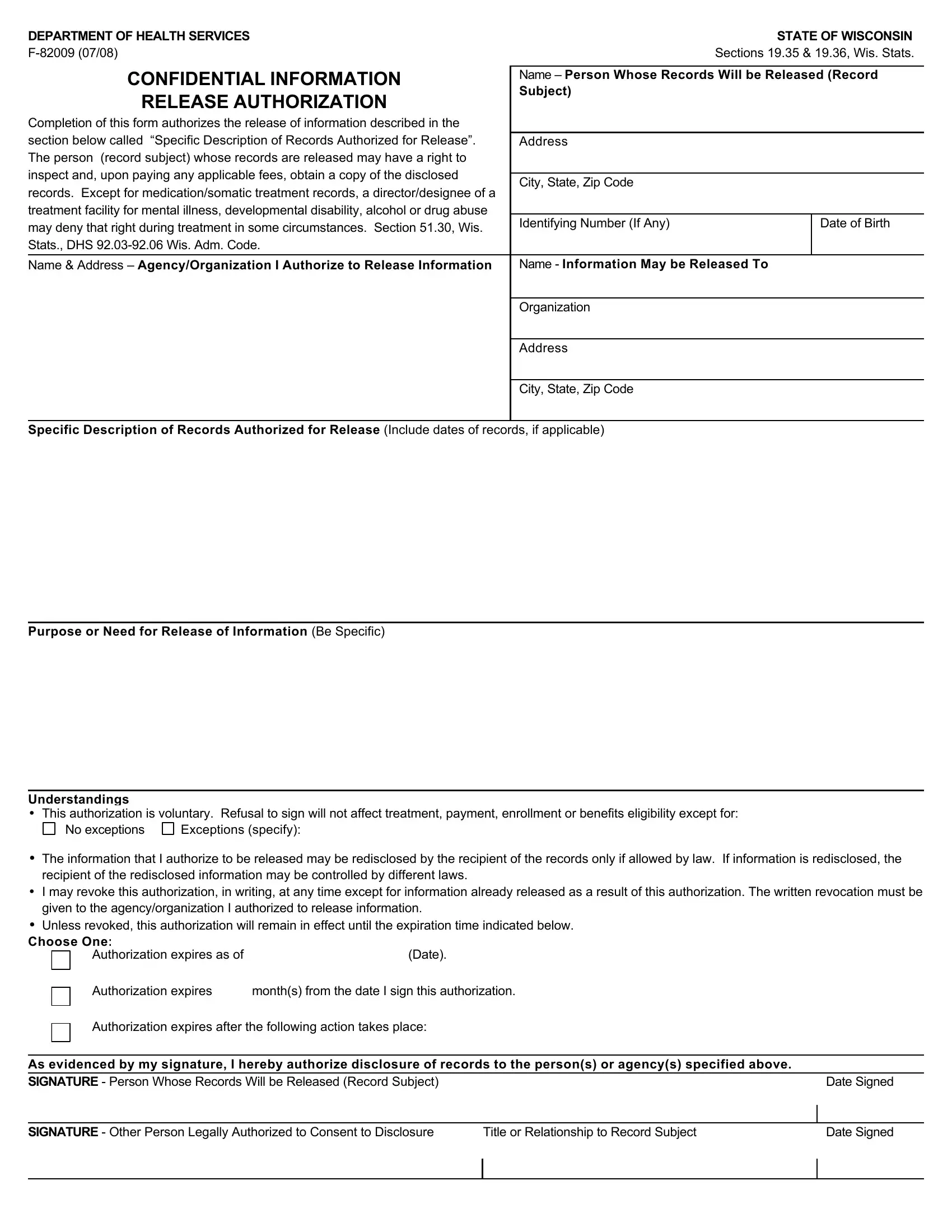
1. Before anything else, while filling out the F 82009 Form, start out with the part containing following blanks:
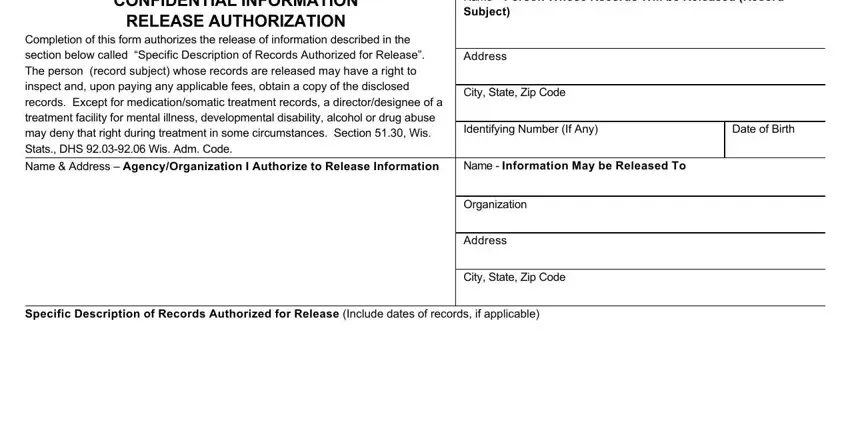
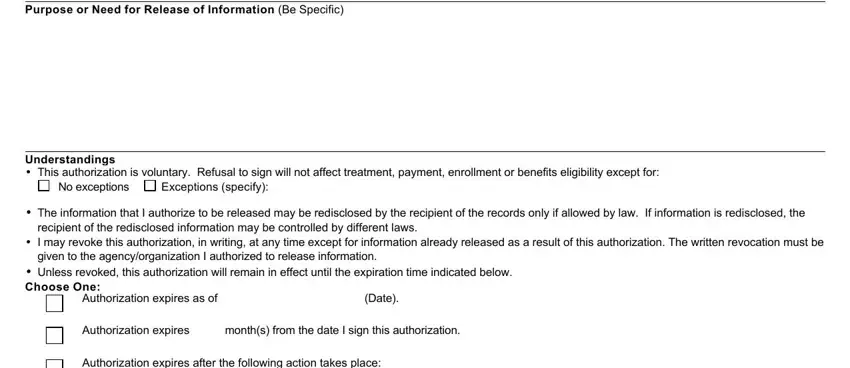
2. When this array of fields is done, you're ready add the needed specifics in Purpose or Need for Release of, Understandings This authorization, No exceptions, Exceptions specify, The information that I authorize, recipient of the redisclosed, I may revoke this authorization, given to the agencyorganization I, Unless revoked this authorization, Authorization expires as of, Date, Authorization expires months from, and Authorization expires after the so you can proceed to the 3rd stage.
3. This next segment is focused on As evidenced by my signature I, Date Signed, SIGNATURE Other Person Legally, Title or Relationship to Record, and Date Signed - fill in these blank fields.

People generally make mistakes while completing Date Signed in this section. Ensure you read twice what you type in here.
Step 3: Once you've glanced through the details in the file's blanks, just click "Done" to finalize your form. Make a free trial subscription with us and get immediate access to F 82009 Form - with all adjustments preserved and available from your personal account. When using FormsPal, you can complete documents without having to get worried about personal data breaches or entries being shared. Our protected software ensures that your private data is kept safe.