
With the help of the online PDF tool by FormsPal, it is possible to fill in or change form mo review form right here. Our tool is constantly developing to present the best user experience achievable, and that is due to our dedication to continuous improvement and listening closely to testimonials. This is what you'd need to do to begin:
Step 1: Firstly, open the pdf editor by clicking the "Get Form Button" at the top of this page.
Step 2: After you access the editor, you'll see the document ready to be filled in. Aside from filling in various blank fields, you could also perform other actions with the file, specifically putting on any text, editing the original textual content, adding images, affixing your signature to the PDF, and more.
Pay attention while filling in this pdf. Make sure all necessary fields are done correctly.
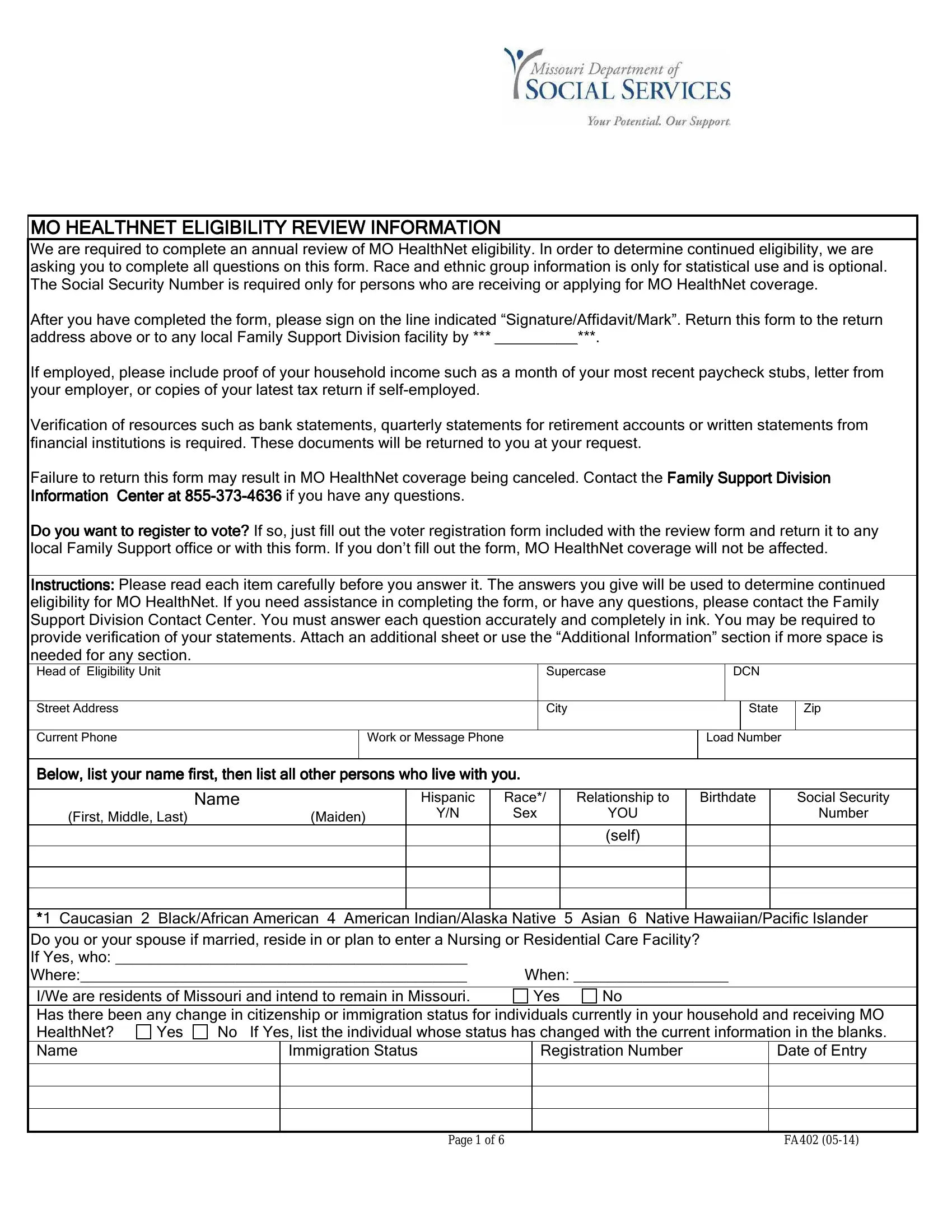
1. Start filling out the form mo review form with a selection of necessary blank fields. Note all of the necessary information and ensure not a single thing missed!
2. Soon after the first section is completed, proceed to type in the relevant information in these: First Middle Last Maiden, Sex, YOU self, Number, Caucasian BlackAfrican American, Registration Number, Immigration Status, Date of Entry, Yes, Yes, and Page of.
Lots of people generally get some things incorrect while filling in Yes in this part. Don't forget to revise whatever you type in right here.
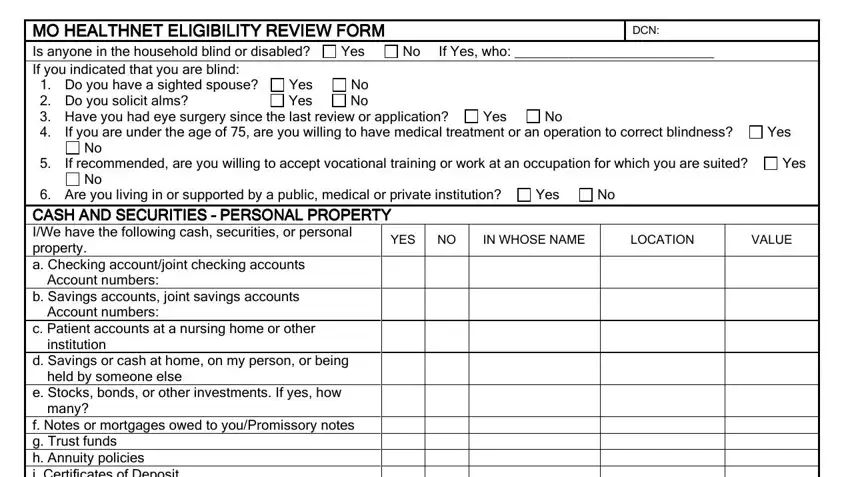
3. Completing MO HEALTHNET ELIGIBILITY REVIEW, Yes Yes, No No, Yes, No If Yes who, DCN, If you are under the age of are, Yes, If recommended are you willing to, Yes, Yes, IN WHOSE NAME, YES, Are you living in or supported by, and LOCATION is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
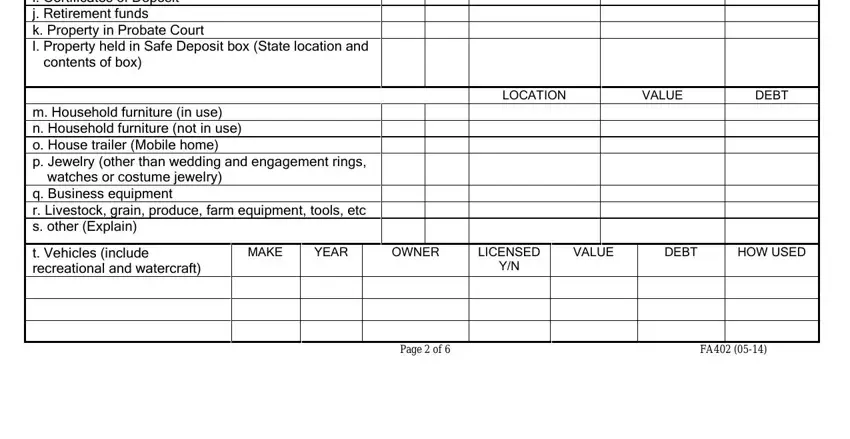
4. Filling out Are you living in or supported by, LOCATION, VALUE, DEBT, m Household furniture in use n, MAKE, YEAR, OWNER, LICENSED, VALUE, DEBT, HOW USED, t Vehicles include recreational, and Page of is essential in the fourth part - don't forget to take the time and be mindful with every field!
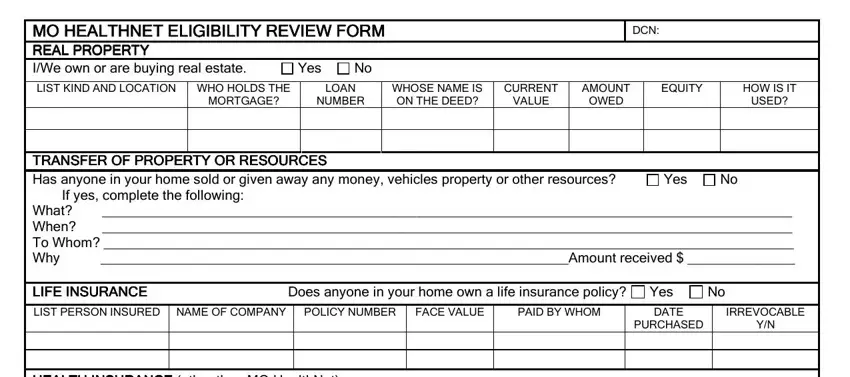
5. Last of all, this final subsection is precisely what you should complete before using the document. The blanks in this case include the next: MO HEALTHNET ELIGIBILITY REVIEW, Yes, DCN, LIST KIND AND LOCATION WHO HOLDS, MORTGAGE, LOAN, NUMBER, WHOSE NAME IS ON THE DEED, CURRENT, VALUE, AMOUNT OWED, EQUITY, HOW IS IT, USED, and TRANSFER OF PROP TRANSFER OF.
Step 3: Immediately after going through your form fields you have filled in, click "Done" and you're done and dusted! Right after setting up a7-day free trial account here, it will be possible to download form mo review form or email it promptly. The document will also be accessible from your personal account with all your modifications. FormsPal is dedicated to the confidentiality of all our users; we make sure all personal data put into our system continues to be secure.