
Using PDF forms online is always a breeze with our PDF tool. Anyone can fill in optum form credentialing application here and use many other options we provide. To make our tool better and more convenient to work with, we constantly come up with new features, with our users' feedback in mind. Should you be seeking to get going, here is what it requires:
Step 1: First, open the pdf editor by pressing the "Get Form Button" above on this site.
Step 2: With our state-of-the-art PDF editor, you'll be able to do more than simply fill out forms. Try all of the functions and make your documents look perfect with customized textual content incorporated, or fine-tune the original input to excellence - all that supported by an ability to incorporate stunning images and sign the PDF off.
This form will need particular details to be entered, hence make sure you take your time to type in precisely what is requested:
1. Complete the optum form credentialing application with a selection of essential fields. Gather all the important information and be sure not a single thing neglected!
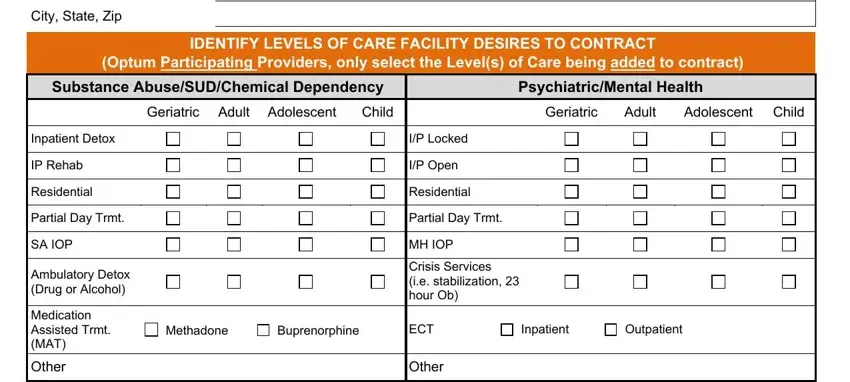
2. Once the last array of fields is completed, you need to insert the needed details in City State Zip, IDENTIFY LEVELS OF CARE FACILITY, Optum Participating Providers only, Substance AbuseSUDChemical, PsychiatricMental Health, Geriatric Adult Adolescent, Child, Geriatric, Adult, Adolescent Child, Inpatient Detox, IP Rehab, Residential, Partial Day Trmt, and SA IOP allowing you to go further.
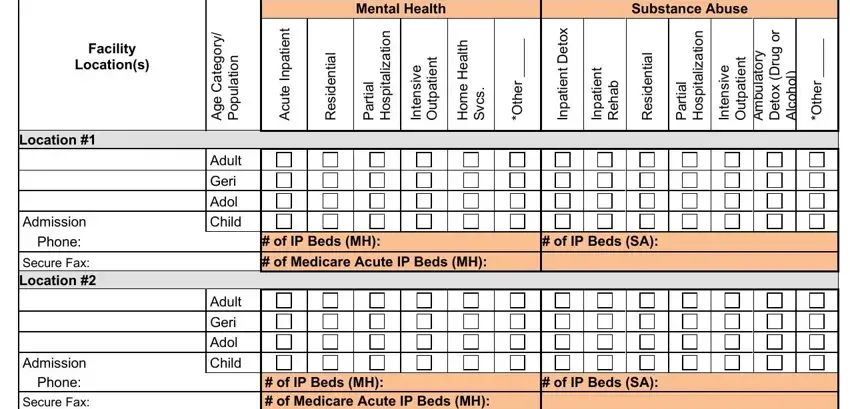
3. The following segment will be focused on Facility, Locations, Location, Admission Phone, Secure Fax Location, Admission Phone Secure Fax, y r o g e t a C e g A, n o i t a u p o P, Adult Geri Adol Child, Adult Geri Adol Child, Mental Health, Substance Abuse, t n e i t a p n I e t u c A, n o i t a z, and i l - complete all of these fields.
4. This next section requires some additional information. Ensure you complete all the necessary fields - Admission Phone Secure Fax, Admission Phone Secure Fax, Admission Phone Secure Fax, Admission Phone Secure Fax, Adult Geri Adol Child, Adult Geri Adol Child, Adult Geri Adol Child, of IP Beds MH of Medicare Acute, of IP Beds SA, of IP Beds MH of Medicare Acute, and of IP Beds SA - to proceed further in your process!
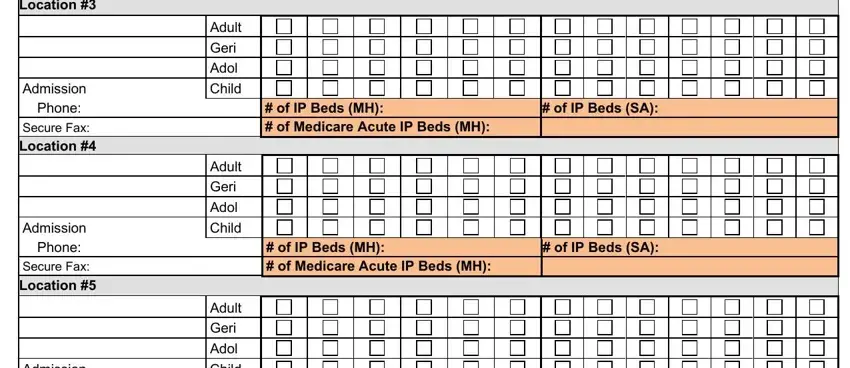
Be very mindful when filling out Adult Geri Adol Child and Adult Geri Adol Child, as this is the section in which many people make some mistakes.
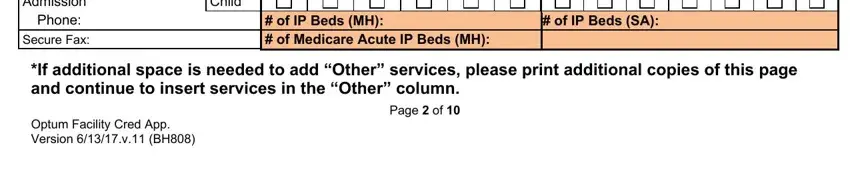
5. The very last step to conclude this PDF form is crucial. You'll want to fill out the necessary fields, like Admission Phone Secure Fax, Adult Geri Adol Child, of IP Beds MH of Medicare Acute, of IP Beds SA, If additional space is needed to, and Optum Facility Cred App Version v, prior to finalizing. Or else, it could contribute to an unfinished and probably unacceptable document!
Step 3: Glance through what you have inserted in the form fields and then click on the "Done" button. After starting afree trial account at FormsPal, it will be possible to download optum form credentialing application or email it without delay. The PDF will also be available from your personal cabinet with your changes. FormsPal is invested in the confidentiality of our users; we make certain that all information entered into our editor is protected.