

If you wish to fill out mg2 form ny workers comp, you don't have to download and install any applications - just give a try to our PDF tool. The tool is continually updated by our staff, receiving handy functions and turning out to be greater. To get the process started, take these basic steps:
Step 1: Firstly, open the editor by clicking the "Get Form Button" above on this page.
Step 2: As soon as you access the online editor, you will see the form prepared to be filled out. Apart from filling in different blanks, you may also perform other actions with the form, that is putting on custom text, changing the original text, inserting graphics, signing the form, and more.
Be attentive while filling in this document. Ensure that each blank field is done correctly.
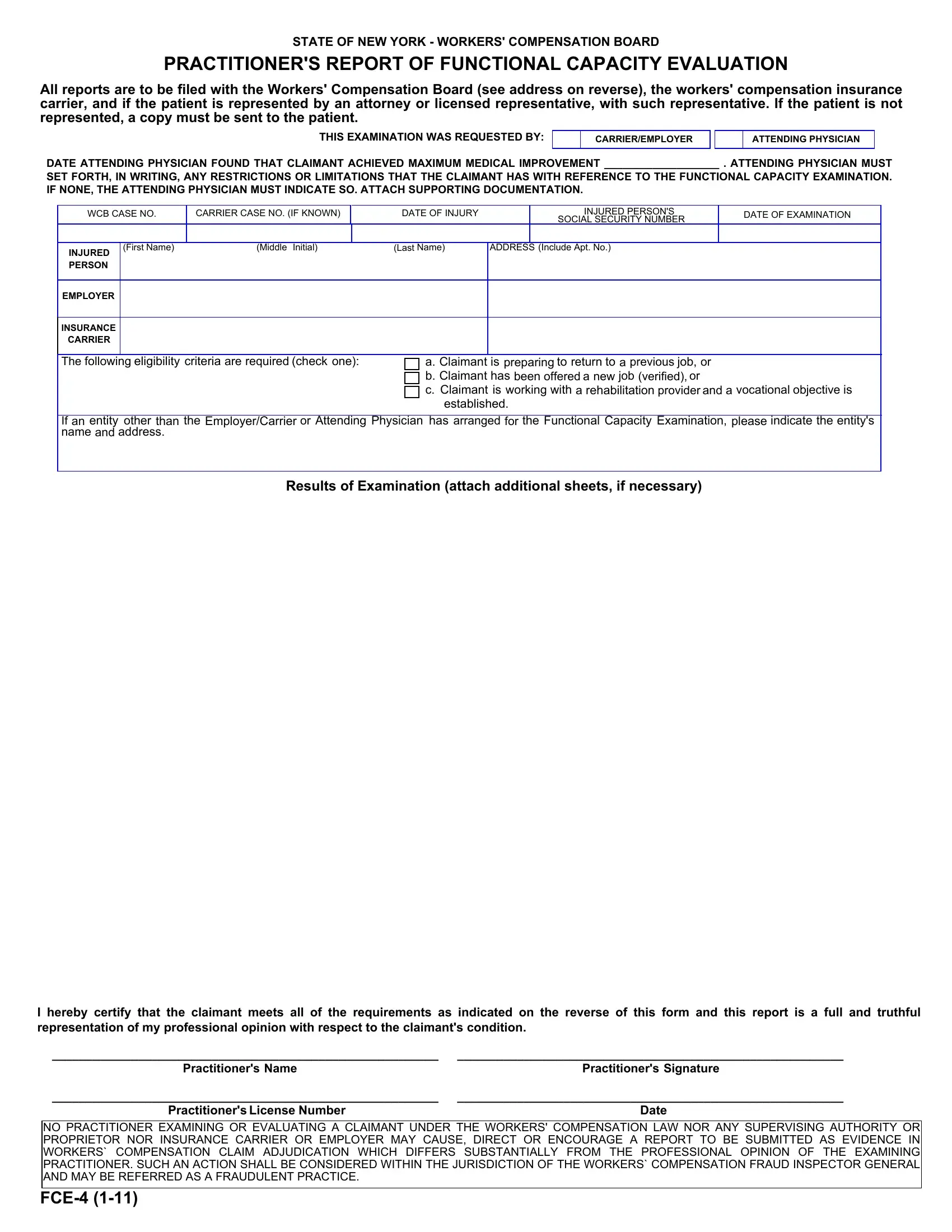
1. The mg2 form ny workers comp requires particular details to be inserted. Make sure the subsequent blank fields are completed:
2. After the last segment is completed, you're ready add the necessary specifics in I hereby certify that the claimant, Practitioners Name, Practitioners Signature, Practitioners License Number, Date, NO PRACTITIONER EXAMINING OR, and FCE so that you can go further.
Be very careful while completing Date and Practitioners Signature, as this is the part where a lot of people make mistakes.
Step 3: Reread everything you have entered into the blank fields and click on the "Done" button. Join us right now and immediately access mg2 form ny workers comp, set for download. All adjustments you make are kept , making it possible to edit the document further when necessary. Whenever you work with FormsPal, you can complete forms without being concerned about personal information leaks or entries getting distributed. Our protected system ensures that your personal information is maintained safe.