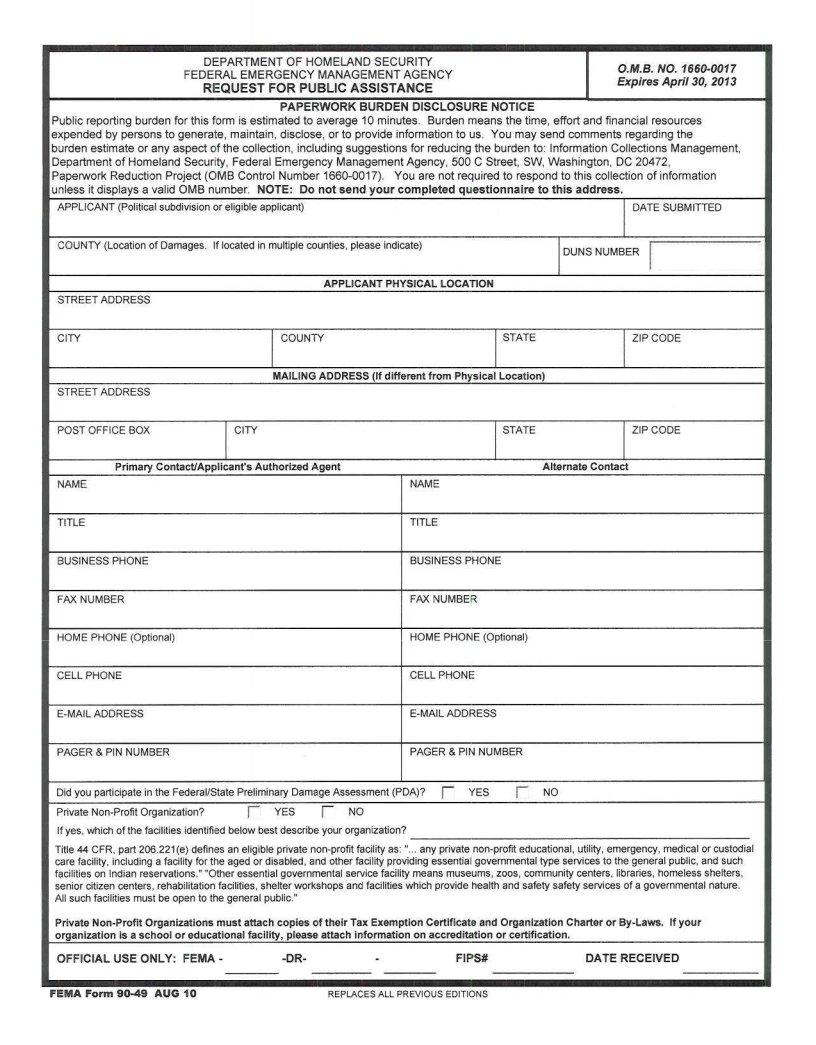
When disasters strike, the need for swift and efficient aid becomes paramount for affected communities. To navigate this critical period, the FEMA Request for Public Assistance (RPA) Form 90-49 serves as a cornerstone for securing essential public assistance funds. It lays the groundwork for governmental entities, Native American Tribal organizations, and specific non-profit organizations to apply for aid under the Stafford Act, which does not guarantee eligibility but signals their interest in the program. This process is initiated with an urgent necessity for applicants to submit their RPA within 30 days following a presidential disaster declaration, a tight deadline underscoring the urgency of disaster recovery efforts. Additionally, applicants are tasked with providing comprehensive information, including but not limited to their federal tax identification, organization charter, and a detailed description of their structural and membership policies. The submission entails a commitment to maintaining a drug-free workplace, a condition that reflects the seriousness with which applicants must approach their request for aid. Not just a formality, the RPA embodies the organizational readiness to undertake the responsibilities that come with disaster relief, including the consolidation of documentation activities and ensuring the completion of necessary work—all while under the stringent guidance of both FEMA and state inquiries. The inclusive checklist accompanying the RPA ensures that potential applicants are well informed of the exhaustive nature of requirements, spotlighting the critical role of this form in the broader context of disaster management and recovery.
| Question | Answer |
|---|---|
| Form Name | Fema Request For Public Assistance Form 90 49 |
| Form Length | 7 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 45 sec |
| Other names | form 90 49, fema rpa form, new york state change of residency checklist, pnp questionnaire |
PNP Checklist
O RPA Form
O Drug Free Workplace Form
O Applicant Certification
O Federal Tax Identification Number Form
O State Tax Exempt Form / IRS Letter
O PNP Questionnaire
OOfficial
O
OOrganization Charter or
OPublications/brochures that describe your organization
ODescription of membership policies or fee structures
INSTRUCTION SHEET
REQUEST FOR PUBLIC ASSISTANCE FORM (RPA)
Submitting the Request for Public Assistance (RPA) form is the initial step in filing for the Public Assistance Program. Any governmental entity (village, town, city, county, or state agency), Native American Tribal Organization, or certain private
Submittal of the RPA does not make an applicant eligible for public assistance under the Stafford Act. The RPA is used by a potential applicant to indicate interest in the Public Assistance Program.
Applicants should make every effort to complete and return their RPA prior to leaving the applicant briefing. The RPA must be submitted within 30 days of the date of the presidential declaration. If a potential applicant fails to submit the RPA within the specified time frame, they may be denied eligibility for public assistance funds.
On the RPA, the applicant must designate their representative or point of contact. The persons named should have the authority of the chief elected official and should be:
Knowledgeable of the work to be inspected,
Knowledgeable of the location of damages,
Easily accessible by telephone (day & evening), and
Available for future FEMA or State inquiries.
The representatives will also have the overall responsibility to:
Consolidate the disaster documentation activities among departments,
Ensure completion of disaster work, and
Submit applicable reporting forms.
Completing the RPA form: All potential applicants must complete the Request for Public Assistance form. At the top of the form fill in the appropriate declaration number. Enter the date the form is completed. Ensure name, address, and telephone numbers are entered (both home and business number).

CERTIFICATION REGARDING DRUG- FREE WORKPLACE REQUIREMENTS
This certification is required by the regulations implementing the
(See 44 CFR Part 17, Subpart C, 17.300, and Subpart D, 17.400)
A. The subgrantee certifies that it will or will not continue to provide a
(a) publishing a statement notifying employees that the unlawful manufacture, distribution, dispersing, possession, or use of a controlled substance is prohibited in the subgrantees workplace and specifying the actions that will be taken against employees for violation of such prohibition;
(b)establishing an ongoing
(1)the dangers of drug abuse in the workplace;
(2)the subgrantees policy of maintaining a
(3)any available drug counseling, rehabilitation, and employee assistance programs;
(4)the penalties that may be imposed upon the employee for drug abuse violations occurring in the workplace;
(c)making it a requirement that each employee to be engaged in the performance of the
(d)notifying the employee in the statement required by paragraph (a) that, as a condition of employment under subgrant, the employee will-
(1)abide by the terms of that statement; and
(2)notify the employer in writing of his or her conviction for a violation of a criminal drug statute occurring in the workplace no later than five calendar days after such conviction;
(e)notifying the New York State Emergency Management Office in writing within ten calendar days after receiving notice under subparagraph (d) (2) from an employee or otherwise receiving actual notice of such conviction. Such notice shall include the position title of the employee and the federal identification number of the subgrantee.
(f)taking one of the following actions, within 30 calendar days of receiving notice under subparagraph (d) (2), with respect to any employee who is so convicted-
(1) taking appropriate personnel action against such an employee, up to and including termination, consistent with the requirements of the Rehabilitation
Act of 1973, as amended; or
(2)requiring such employee to participate satisfactorily in a drug abuse assistance or rehabilitation program approved for such purposes by a Federal, State, or local health, law enforcement, or other appropriate agency;
(g)making a good faith effort to continue to maintain a
B.The subgrantee may insert in the space provided below the site (s) for the performance of work done in connection with this grant:
Place (s) of Performance: (Please PRINT in the Street address, city, county, state and zip code)
Organization Name: ________________________________________________ Disaster Name: FEMA-
(Please Print ) Name and Title of Authorized Representative:______________________________________________________
Signature:_________________________________________________________Date:___________________________________
New York State Office of Emergency Management
PRESIDENTIAL DECLARATION
STATE OFFICE of EMERGENCY MANAGEMENT
APPLICANT CERTIFICATION
This is to certify the receipt of the guidelines, and associated documents for the Presidential Declaration as administered by the State Office of Emergency Management (SOEM).
The signature below indicates the intent of the (circle one and PRINT in the name):
County City Town Village State Agency School Fire District
of __________________________________________________________________, hereinafter referred
to as the subgrantee, to participate in the Presidential Declaration
The public assistance program is voluntary. It is understood that by choosing to participate in the grant program, the subgrantee is responsible to: 1) comply with all federal and state laws, regulations, policies, and procedures; 2) fulfill the eligibility requirements to participate as a subgrantee of the State; and 3) certify that all figures to be provided in the application are true and correct for costs associated with the declaration provisions.
If debris removal is authorized, the subgrantee agrees to indemnify and hold harmless the State of New York and the United States of America for any claims arising from the removal of debris or wreckage for this disaster. The
The undersigned agrees to participate in this program and certifies that to the best of their knowledge and belief, all work and costs claimed are eligible in accordance with the grant conditions and all work claimed has been or will be completed.
SIGNED: ______________________________________ |
DATE: ____________________________ |
CHIEF EXECUTIVE OFFICER |
|
NAME: ________________________________________ |
PHONE NO.: |
Please type or print name/address |
|
ADDRESS: __________________________________________________________________________
CITY,STATE: _____________________________________________ ZIP CODE: ________________
Designation of the Point of Contact if different from above:
NAME: ________________________________________ PHONE NO.:
Please type or print name
TITLE &
ADDRESS: ________________________________________________________________________
FEDERAL TAX IDENTIFICATION NUMBER
(Not for use by State Agencies or Local Political
Disaster No.
In order to process your payment for disaster assistance funds, the State Office of Emergency Management will need to provide the State Comptroller’s Office with your
PAYEE IDENTIFICATION NUMBER.
For an individual, the Payee ID is the social security number. For corporations, including private
Individual:
Business:
Federal Tax ID # :____________________________________
Applicant Name:_____________________________________
Applicant Address:____________________________________
City, Zip Code:_______________________________________
Telephone #:_________________________________________
Signature:____________________________ Date:___________
Please provide this number, as it will assist us in providing
your funding in a timely manner.
Please mail or fax it, as soon as possible, to:
Recovery Section
State Office of Emergency Management
1220 Washington Avenue
Building 22, Suite 101
Albany, New York
Fax:
FEDERAL EMERGENCY MANAGEMENT AGENCY
PNP FACILITY QUESTIONNAIRE
This questionnaire is to be used by FEMA and state personnel to help determine the eligibility of specific facilities of an approved Private
Name of PNP Organization:
Name of the damaged facility and location:
What is the primary purpose of the damaged facility?
Who may use this facility?
What fee, if any, is charged for the use of the facility?
Was the facility in use at the time of the disaster? |
Yes |
No |
|
Did the facility sustain damage as a direct result of the disaster? |
Yes |
No |
|
What type of assistance is being requested? |
|
|
|
Does the PNP organization own the facility?
Yes
No
If "Yes," obtain proof of ownership; check here if attached.
If "No," do they lease / rent the facility?
Yes
No
If "Yes," obtain a copy of the lease or rental agreement for the damaged facility; check here if attached.
Are the repairs of this facility the legal responsibility of the organization?
Yes
No
Is the facility insured?
Yes
No
If "Yes," obtain a copy of the insurance policy; check here if attached.
Additional information or comments:
Name of contact person
Phone number
FEMA FORM