

Using PDF forms online is always simple with this PDF editor. You can fill out compassionate usnon program here painlessly. To keep our tool on the forefront of practicality, we strive to adopt user-oriented capabilities and improvements regularly. We are always grateful for any suggestions - assist us with reshaping how you work with PDF documents. By taking a few basic steps, you are able to start your PDF journey:
Step 1: Click on the "Get Form" button in the top section of this page to open our PDF tool.
Step 2: The editor will give you the opportunity to modify PDF documents in a variety of ways. Modify it by including any text, correct what's already in the PDF, and include a signature - all within the reach of a couple of clicks!
As for the fields of this particular PDF, here is what you should consider:
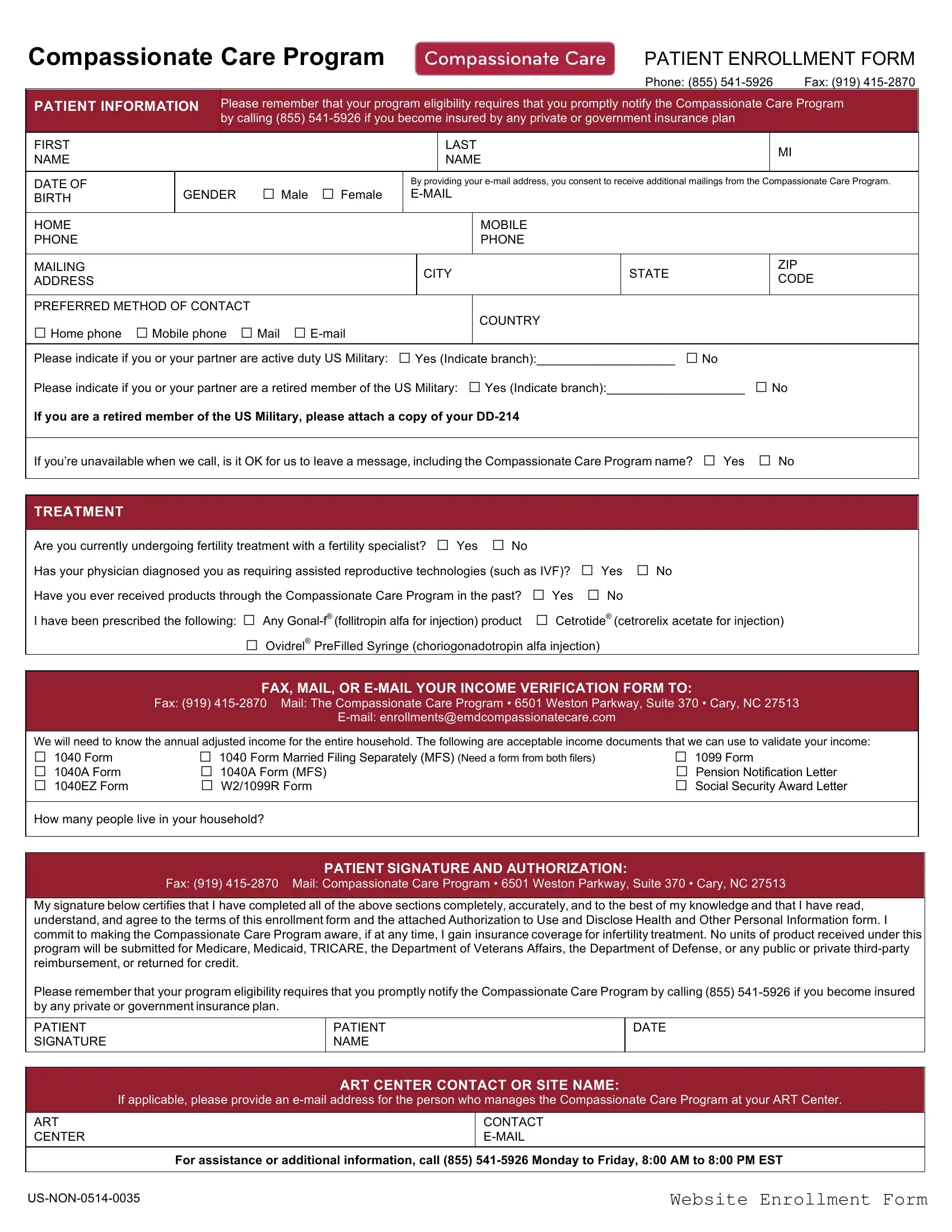
1. While filling out the compassionate usnon program, make certain to incorporate all needed fields in its relevant form section. This will help facilitate the process, making it possible for your details to be processed quickly and properly.
2. Just after the previous section is done, go to enter the relevant details in all these - Are you currently undergoing, Fax Mail The Compassionate Care, FAX MAIL OR EMAIL YOUR INCOME, Email, We will need to know the annual, How many people live in your, Fax Mail Compassionate Care, PATIENT SIGNATURE AND AUTHORIZATION, My signature below certifies that, PATIENT NAME, and DATE.
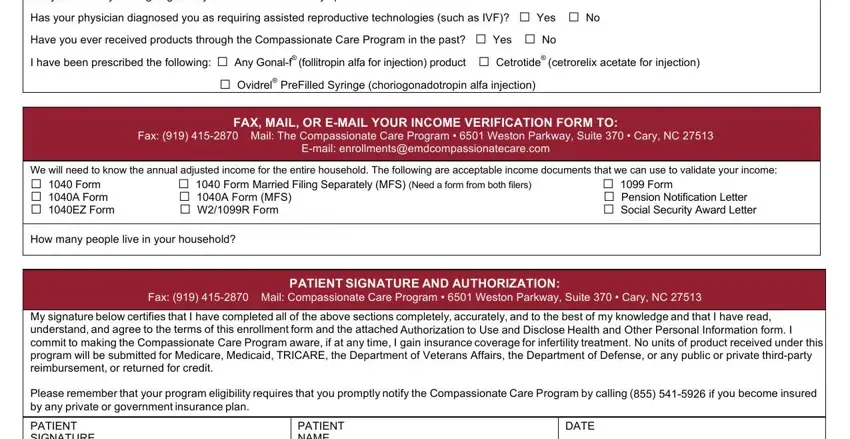
As to Are you currently undergoing and FAX MAIL OR EMAIL YOUR INCOME, make sure you do everything right in this section. These two are viewed as the key ones in this document.
3. The next part should also be fairly uncomplicated, If applicable please provide an, ART CENTER CONTACT OR SITE NAME, ART CENTER, CONTACT EMAIL, For assistance or additional, USNON, and Website Enrollment Form - all these empty fields needs to be filled in here.

4. Filling in Authorization to Use and Disclose, Patients Name, Address, Home Phone, DOB, I authorize my physician and, contact me by mail email andor, Seronos Compassionate Care Program, and provide me with materials is key in this fourth step - make certain that you be patient and fill out every blank!
5. The pdf must be wrapped up by filling in this segment. Here there is a comprehensive list of blank fields that must be filled in with correct information for your document usage to be complete: Patient name please print, Signature of patient or personal, Date, Authorityrelationship of personal, Signature of patient or personal, Date, and Authorityrelationship of personal.
Step 3: Soon after looking through your fields, hit "Done" and you're good to go! Sign up with FormsPal now and easily gain access to compassionate usnon program, all set for download. All adjustments made by you are kept , making it possible to edit the document further when required. We do not share the details you use whenever completing documents at FormsPal.