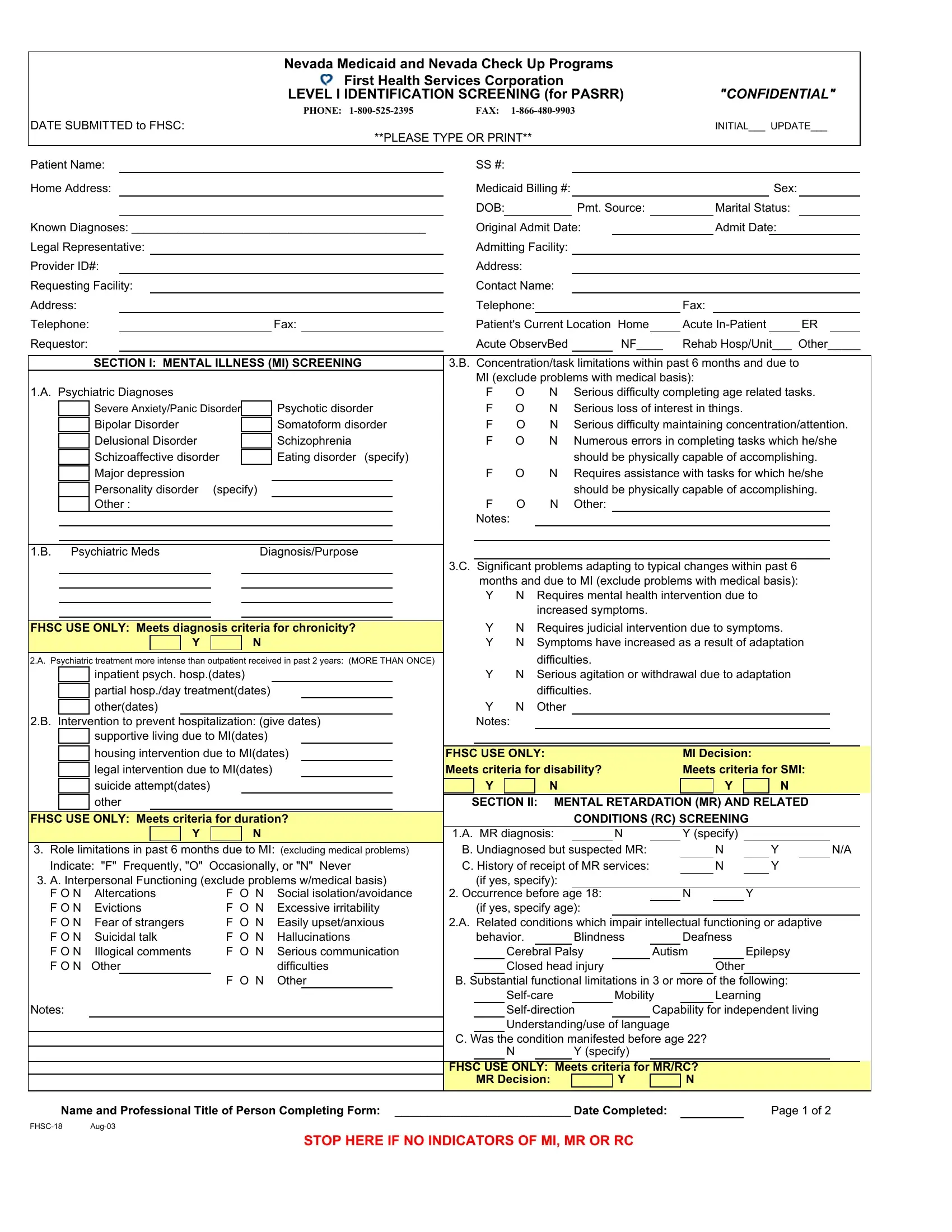
The Fhsc 18 Nevada form plays a crucial role within the Nevada Medicaid and Nevada Check Up Programs operated by First Health Services Corporation, serving as a primary tool for Level I Identification Screening in accordance with the Pre-Admission Screening and Resident Review (PASRR). This comprehensive form is designed to ensure that individuals seeking admission into Medicaid-funded nursing facilities or requiring specialized services due to mental illness (MI), mental retardation (MR), related conditions (RC), or dementia are appropriately evaluated. The sections within the form cover extensive ground, including mental illness screening and interventions, determinations for mental retardation and related conditions, dementia assessment, and categorical determinations for conditions such as terminal illness and severe physical illness. Moreover, the form assesses the need for exempted hospital discharge and time-limited categorical determinations, crucial steps in facilitating the right care pathways. The confidentiality underscored by this process ensures sensitive patient information is handled with the utmost care, maintaining dignity and respect for the individuals and their families navigating these complex systems.
| Question | Answer |
|---|---|
| Form Name | Fhsc 18 Form Nevada |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Requestor, PASRR, NF, IIE |

|
|
|
|
|
|
|
|
|
Nevada Medicaid and Nevada Check Up Programs |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
First Health Services Corporation |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
LEVEL I IDENTIFICATION SCREENING (for PASRR) |
|
"CONFIDENTIAL" |
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
PHONE: |
|
FAX: |
|
|
|
|
|
|
|
|
|
|
|||||
DATE SUBMITTED to FHSC: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INITIAL___ UPDATE___ |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
**PLEASE TYPE OR PRINT** |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Patient Name: |
|
|
|
|
|
|
|
|
SS #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Home Address: |
|
|
|
|
|
|
|
|
Medicaid Billing #: |
|
|
|
|
|
|
Sex: |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
DOB: |
|
|
|
Pmt. Source: |
|
Marital Status: |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Known Diagnoses: _____________________________________________ |
|
Original Admit Date: |
|
|
|
Admit Date: |
|
|
|
|
|||||||||||||||||
Legal Representative: |
|
|
|
|
|
|
|
|
Admitting Facility: |
|
|
|
|
|
|
|
|
|
|
|
|||||||
Provider ID#: |
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Requesting Facility: |
|
|
|
|
|
|
|
Contact Name: |
|
|
|
|
|
|
|
|
|
|
|||||||||
Address: |
|
|
|
|
|
|
|
|
|
|
|
Telephone: |
|
|
|
|
|
Fax: |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone: |
|
|
|
|
|
|
|
Fax: |
|
|
Patient's Current Location |
Home |
|
Acute |
|
ER |
|
|
|||||||||
Requestor: |
|
|
|
|
|
|
|
|
|
|
|
Acute ObservBed |
|
NF____ |
Rehab Hosp/Unit___ Other_____ |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
SECTION I: MENTAL ILLNESS (MI) SCREENING |
3.B. Concentration/task limitations within past 6 months and due to |
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
MI (exclude problems with medical basis): |
|
|
|
|
|
|
||||||||
1.A. Psychiatric Diagnoses |
|
|
|
|
|
|
|
F |
O |
N Serious difficulty completing age related tasks. |
|||||||||||||||||
|
|
Severe Anxiety/Panic Disorder |
|
|
Psychotic disorder |
|
F |
O |
N Serious loss of interest in things. |
|
|
|
|
|
|
||||||||||||
|
|
Bipolar Disorder |
|
|
|
Somatoform disorder |
|
F |
O |
N Serious difficulty maintaining concentration/attention. |
|||||||||||||||||
|
|
Delusional Disorder |
|
|
|
Schizophrenia |
|
F |
O |
N Numerous errors in completing tasks which he/she |
|||||||||||||||||
|
|
Schizoaffective disorder |
|
|
Eating disorder (specify) |
|
|
|
|
|
should be physically capable of accomplishing. |
||||||||||||||||
|
|
Major depression |
|
|
|
|
|
|
|
F |
O |
N Requires assistance with tasks for which he/she |
|||||||||||||||
|
|
Personality disorder |
(specify) |
|
|
|
|
|
|
|
|
should be physically capable of accomplishing. |
|||||||||||||||
|
|
Other : |
|
|
|
|
|
|
|
F |
O |
N Other: |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Notes: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
1.B. Psychiatric Meds |
|
|
Diagnosis/Purpose |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
3.C. Significant problems adapting to typical changes within past 6 |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
months and due to MI (exclude problems with medical basis): |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
N |
Requires mental health intervention due to |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
increased symptoms. |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FHSC USE ONLY: Meets diagnosis criteria for chronicity? |
|
Y |
N |
Requires judicial intervention due to symptoms. |
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
Y |
|
|
N |
|
|
|
|
Y |
N |
Symptoms have increased as a result of adaptation |
||||||||||||
2.A. Psychiatric treatment more intense than outpatient received in past 2 years: (MORE THAN ONCE) |
|
|
|
difficulties. |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
inpatient psych. hosp.(dates) |
|
|
|
|
|
Y |
N |
Serious agitation or withdrawal due to adaptation |
|
|
|
|
|||||||||||||
|
|
partial hosp./day treatment(dates) |
|
|
|
|
|
|
difficulties. |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
other(dates) |
|
|
|
|
|
|
|
|
Y |
N |
Other |
|
|
|
|
|
|
|
|
|
|
|
|||
2.B. Intervention to prevent hospitalization: (give dates) |
|
Notes: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
supportive living due to MI(dates) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
housing intervention due to MI(dates) |
FHSC USE ONLY: |
|
|
MI Decision: |
|
|
|
|
|||||||||||||||||
|
|
legal intervention due to MI(dates) |
|
|
|
Meets criteria for disability? |
|
|
Meets criteria for SMI: |
||||||||||||||||||
|
|
suicide attempt(dates) |
|
|
|
|
|
|
Y |
|
N |
|
|
|
Y |
|
N |
|
|
|
|
||||||
|
|
other |
|
|
|
|
|
|
SECTION II: MENTAL RETARDATION (MR) AND RELATED |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FHSC USE ONLY: Meets criteria for duration? |
|
|
|
|
|
CONDITIONS (RC) SCREENING |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
Y |
|
|
N |
|
|
|
1.A. MR diagnosis: |
|
N |
|
Y (specify) |
|
|
|
|
|
|
|||||
3. Role limitations in past 6 months due to MI: (excluding medical problems) |
B. Undiagnosed but suspected MR: |
|
N |
|
Y |
|
|
N/A |
|||||||||||||||||||
Indicate: "F" Frequently, "O" |
Occasionally, or "N" Never |
C. History of receipt of MR services: |
|
N |
|
Y |
|
|
|
|
|||||||||||||||||
3. A. Interpersonal Functioning (exclude problems w/medical basis) |
|
(if yes, specify): |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
F O N |
Altercations |
F |
O |
N |
Social isolation/avoidance |
2. Occurrence before age 18: |
|
|
N |
Y |
|
|
|
|
|||||||||||||
F O N |
Evictions |
F |
O |
N |
Excessive irritability |
|
(if yes, specify age): |
|
|
|
|
|
|
|
|
|
|
||||||||||
F O N Fear of strangers |
F |
O |
N |
Easily upset/anxious |
2.A. Related conditions which impair intellectual functioning or adaptive |
||||||||||||||||||||||
F O N Suicidal talk |
F |
O |
N |
Hallucinations |
|
behavior. |
|
|
Blindness |
|
Deafness |
|
|
|
|
|
|
||||||||||
F O N Illogical comments |
F O N |
Serious communication |
|
|
Cerebral Palsy |
|
Autism |
Epilepsy |
|
|
|
|
|||||||||||||||
F O N |
Other |
|
|
|
difficulties |
|
|
Closed head injury |
|
|
|
Other |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
F |
O |
N |
Other |
B. Substantial functional limitations in 3 or more of the following: |
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mobility |
|
Learning |
|
|
|
|
||||||
Notes: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Capability for independent living |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Understanding/use of language |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
C. Was the condition manifested before age 22? |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
Y (specify) |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FHSC USE ONLY: Meets criteria for MR/RC? |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
MR Decision: |
|
|
Y |
|
N |
|
|
|
|
|
|
|||
|
Name and Professional Title of Person Completing Form: ___________________________ Date Completed: |
|
|
|
Page 1 of 2 |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
STOP HERE IF NO INDICATORS OF MI, MR OR RC |
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

|
|
|
|
|
|
|
|
|
|
|
Nevada Medicaid and Check Up Program |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
First Health Services Corporation |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
LEVEL I IDENTIFICATION SCREENING (for PASRR) |
|
"CONFIDENTIAL" |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
STOP HERE - IF NO INDICATORS OF MI, MR OR RC |
|
SECTION VI: OTHER CATEGORICAL |
||||||||||||||||||||||||
|
|
|
|
OTHERWISE CONTINUE |
|
|
|
|
IIF. |
|
Terminal Illness: Physician has certified life expectancy of less |
|||||||||||||||
SECTION III: DEMENTIA |
(complete for both MI & MR/RC) |
|
|
|
than 6 months. (Submit copy of certification). |
|||||||||||||||||||||
A. Does the individual have a primary diagnosis of Dementia or |
|
IIG. |
|
Severe Physical Illness limited to: |
|
|
|
|||||||||||||||||||
Alzheimer's Disease? |
|
|
|
|
|
|
|
|
|
|
|
|
Coma, Ventilator Dependence, functioning at a brain stem level |
|||||||||||||
|
|
|
Y |
|
N (specify) |
|
|
|
|
|
|
|
|
|
|
|
|
or a diagnosis of Parkinson's, Chronic Obstructive Pulmonary |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
B. Does the individual have any other organic disorders? |
|
|
|
|
|
|
Disease, Huntington's disease, Amyotrophic lateral sclerosis |
|||||||||||||||||||
|
|
|
Y |
|
N (specify) |
|
|
|
|
|
|
|
|
|
|
|
|
or congestive heart failure which result in a level of |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
C. Is there evidence of undiagnosed Dementia or other organic |
|
|
|
impairment so severe that the individual could not be expected |
||||||||||||||||||||||
mental disorders? |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
to benefit from specialized services. |
|
|
|
||||||||
Y |
N |
disoriented to time |
Y |
N |
disoriented to situation |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Y |
N disoriented to place |
Y |
N |
pervasive, significant confusion |
FHSC USE ONLY: |
|
|
|
|
|
|
|||||||||||||||
Y N severe ST memory |
Y N paranoid ideation |
|
|
|
|
Meets Other Categorical Determination criteria? |
||||||||||||||||||||
|
|
deficit |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
|
N |
|
|
|
|
|
||
D. Is there evidence of affective symptoms which might be confused |
|
SECTION VII: REQUESTING PROVIDER TO COMPLETE |
||||||||||||||||||||||||
with Dementia? |
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Information (required if indicators of MI, MR/RC): |
|||||||||||||
Y |
N |
frequent tearfulness |
Y |
N |
severe sleep disturbance |
|
|
|
Legal representative's name and address: |
|||||||||||||||||
Y |
N |
frequent anxiety |
Y |
N |
severe appetite disturbance |
|
|
|
|
|
|
|
|
|
|
|
||||||||||
E. Can the requstor provide any corroborative information to affirm that the |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
dementing condition exists and is the primary diagnosis? |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
Dementia |
|
|
Thorough mental status exam |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
____ Medical/functional history prior to onset of dementia |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Primary physician's name and address: |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
STOP - If Dementia is primary to MI. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
CONTINUE - for all MR/RC or |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
FHSC USE ONLY: Meets dementia criteria? |
|
|
Y |
|
|
N |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
SECTION IV: EXEMPTED HOSPITAL DISCHARGE (EHD)* |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
A. Does the individual meet all of the following criteria? |
|
|
|
|
|
|
Additional supporting documentation is attached/submitted. |
|||||||||||||||||||
|
|
|
Admission to a NF directly from a hospital after receiving |
|
|
|
Physician's certification stating a less than 30 day nursing facility |
|||||||||||||||||||
|
|
|
acute |
|
|
|
|
|
|
stay is needed to justify EHD is attached/submiited. |
||||||||||||||||
|
|
|
Requires NF services for the condition he/she received care in |
|
|
Physician's certification for a less than six (6) month life |
||||||||||||||||||||
|
|
|
the hospital; and |
|
|
|
|
|
|
|
|
|
|
|
|
expectancy for terminal illness is attached/submitted. |
||||||||||
|
|
|
The attending physician has certified prior to NF |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
admission that the individual will require less than 30 days |
|
Date Form Completed: |
|
|
|
|
|
|
|||||||||||||||
|
|
|
NF services. (Submit copy) |
|
|
|
|
|
|
|
|
Name and Professional Title of Person Completing form: |
||||||||||||||
* Individuals meeting all above criteria are exempt from PASRR II |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
screening for 30 days. The receiving facility must submit a Level I |
FHSC OFFICE USE ONLY: |
|
|
|
|
|
||||||||||||||||||||
by the 25th day to request PASRR Level II, when it is apparent |
|
SUMMARY and DETERMINATION |
|
|
|
|||||||||||||||||||||
the stay will exceed 30 days. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
FHSC USE ONLY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Has indicators of MI, MR/RC |
|
|
No indicators of MI, |
||||||||
Meets EHD criteria? |
|
Y |
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
MR/RC |
|||||||||
Limitation Date: |
|
|
|
|
|
|
|
|
|
|
|
|
Level I Identification Determination: |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
PASRR LEVEL II CATEGORICAL DETERMINATIONS |
|
|
|
IA - Exempted Hospital Discharge |
|
|
|
|||||||||||||||||||
SECTION V: |
|
|
|
IA - Qualifies for Categorical Determination |
||||||||||||||||||||||
IIE. The following categories indicate the individual requires NF services |
|
|
IA - Requires PASRR Level II Individual Evaluation |
|||||||||||||||||||||||
and does not require specialized services for the time specified. |
|
|
|
IB - Has Dementia, Alzheimer's, Organic Brain Syndrome |
||||||||||||||||||||||
A. _____ Convalescent care from an acute physical illness which |
|
|
|
IC - Not MI, MR/RC or Demented |
|
|
|
|||||||||||||||||||
|
required hospitalization and does not meet all criteria for an EHD. |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
B. |
|
|
Emergency protective service situation for MI or MR/RC |
|
PASRR Level II Categorical Determination: |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
individual - placement in NF not to exceed 7 days. |
|
|
|
|
|
|
PAS (applicant to NF) |
|
|
RR (resident in NF) |
|||||||||||||||
C. |
|
|
Delirium precludes the ability to accurately diagnose. Facility |
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
must obtain PASRR Level II as soon as the delirium clears. |
|
|
|
IIE - Time Limited Approval Limitation Date: ________ |
|||||||||||||||||||||
D. |
|
|
Respite is needed for |
|
|
|
IIF - Terminal Illness |
|
|
|
|
|
||||||||||||||
|
MR/RC individual will return. |
|
|
|
|
|
|
|
|
|
|
|
|
IIG - Severe Physical Illness |
|
|
|
|||||||||
*If any of the above are checked, receiving facility must submit a |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
new Level I to request PASRR Level II ten (10) days prior to the |
|
Referral Needed for PASRR Level II Individual Evaluation: |
||||||||||||||||||||||||
limitation date listed below for resident's whose stay is anticipated |
|
|
Referred for MI |
Date Referred: |
|
|
||||||||||||||||||||
to exceed that date. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Referred for MR/RC |
Date Referred: |
|
|
||||||||
FHSC USE ONLY: Meets IIE Categorical Determination Criteria? |
|
|
|
Dual Referral MI and MR/RC |
Date: |
|||||||||||||||||||||
A. |
|
|
Y |
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. |
Appropriate for NF |
|
Y |
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
Limited to: ____________________ |
|
|
|
|
|
Date Completed |
FHSC Reviewer's Name/Signature |
||||||||||||||||||
Note: Limitations for Convalescent care = 45 days, Emergency Protective Services = 7 days, |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
Delirium = 30 days, and Respite = 30 days. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Jul 2003 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Page 2 of 2 |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|