
 Phone #:
Phone #:
Our best web programmers have worked together to make the PDF editor that you're going to use. This software makes it easy to fill in printable file of life form files instantly and conveniently. This is certainly everything you should do.
Step 1: Choose the button "Get Form Here" and hit it.
Step 2: After you've entered the editing page printable file of life form, you will be able to discover every one of the options available for the form within the upper menu.
Fill in all of the following sections to fill in the form:
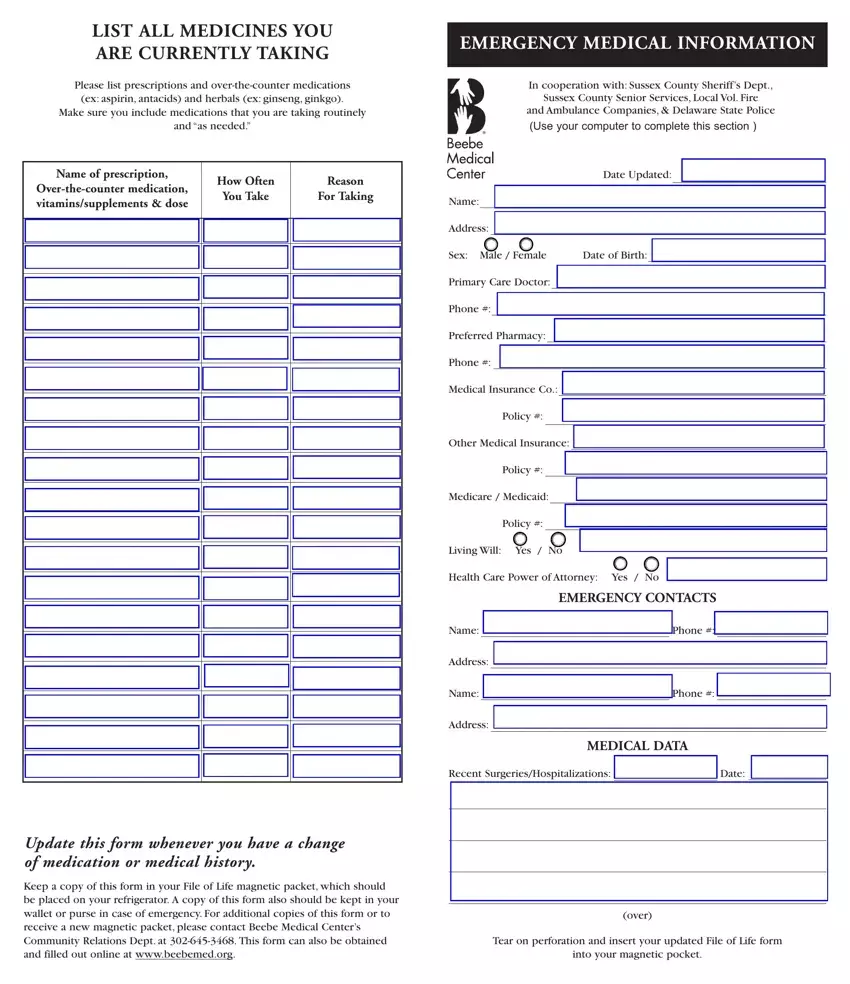
The application will require you to complete the Living Will Yes No, Health Care Power of Attorney Yes, EMERGENCY CONTACTS, Name, Address, Name, Address, Phone, Phone, MEDICAL DATA, Recent SurgeriesHospitalizations, Date, Update this form whenever you have, Keep a copy of this form in your, and over segment.
You have to include specific details within the box Date Updated, Name, Address, Sex Male Female, Date of Birth, Primary Care Doctor, Phone, Preferred Pharmacy, Phone, Medical Insurance Co, Policy, Other Medical Insurance, Policy, Medicare Medicaid, and HEART DISEASE.
The Medicare Medicaid, Policy, MEDICINE ALLERGIESREACTIONS, Drug, Reaction, Blood in Stools, ENDOCRINE DISEASE Diabetes, Thyroid, High, Low, Aspirin, Barbiturates, Codeine, Demerol, and Insect Stings area will be applied to provide the rights or responsibilities of both sides.
Fill in the template by analyzing the following fields: Vaccines, Update this form whenever you have, and Keep a copy of this form in your.
Step 3: Select the "Done" button. Now it's easy to upload your PDF form to your electronic device. Aside from that, you may forward it through email.
Step 4: Ensure that you avoid potential difficulties by preparing a minimum of 2 duplicates of the form.
