
You'll be able to fill out florida hospital discharge instantly in our online PDF editor. Our professional team is ceaselessly working to develop the editor and help it become even faster for people with its many features. Uncover an ceaselessly innovative experience now - take a look at and uncover new possibilities as you go! Should you be looking to get started, here's what it requires:
Step 1: Open the PDF file inside our editor by clicking the "Get Form Button" above on this webpage.
Step 2: The editor offers you the opportunity to change your PDF form in a variety of ways. Enhance it by adding your own text, adjust what is originally in the PDF, and put in a signature - all at your fingertips!
When it comes to blank fields of this particular PDF, here is what you want to do:
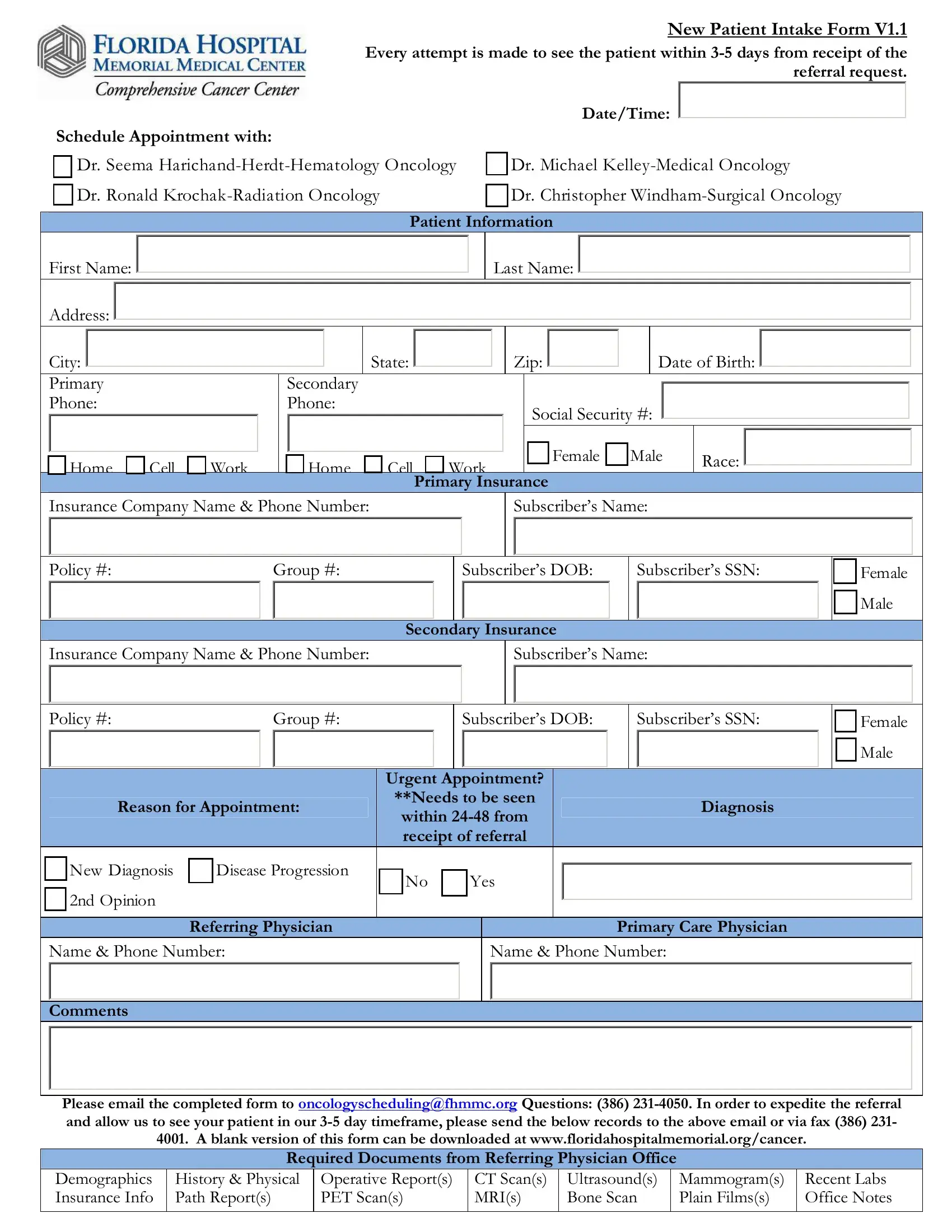
1. First of all, when filling out the florida hospital discharge, start with the part that features the next fields:
2. Once the last array of fields is done, you need to put in the necessary details in Policy, Group, Subscribers DOB, Subscribers SSN, Insurance Company Name Phone, Subscribers Name, Secondary Insurance, Policy, Group, Subscribers DOB, Subscribers SSN, Reason for Appointment, Urgent Appointment Needs to be, Diagnosis, and New Diagnosis nd Opinion so that you can proceed further.
3. This third part is generally easy - fill in all of the empty fields in THIS SECTION TO BE COMPLETED BY, PATIENT INFORMATION, Patient Label, First Name APPOINTMENT DATETIME, Last Name, CARE NAVIGATORS NOTIFIED, Breast Care Navigator Lung Care, Appt Date, Appt Time, PATIENT AND APPOINTMENT ENTERED, Radiation Oncology Dr Krochak, Dr Harichand Dr Kelley Dr Windham, FIN, Cerner Scheduling PATIENT NOTIFIED, and IMPAC to complete this segment.
People often make errors while filling in Appt Date in this part. Be certain to review everything you enter here.
4. The following subsection arrives with the following form blanks to focus on: DateTime Patient Notified, CCC General Pt Packet CWSkin, CWSoft Tissue, CWGeneral, CWBreast CWPort Placement, Spoke directly to patient Spoke, Mailed DateTime, Emailed Email Address, RECORDS RECEIVED FROM REFERRING, Pathology Report, Operative Report, Date, Time, Initials, and Bone Scan.
5. The document should be wrapped up by filling out this area. Further you will see a detailed listing of form fields that have to be completed with accurate information to allow your form submission to be faultless: Chart Label printed Name MRN, CHART FORWARDED TO NURSING, Initials, DateTime, Notes, Chart Label printed Name DOB, DateTime, NURSING RECEIVED, and Initials.
Step 3: Proofread everything you've inserted in the blank fields and click on the "Done" button. After getting a7-day free trial account with us, it will be possible to download florida hospital discharge or email it at once. The PDF file will also be readily accessible via your personal account page with your every single modification. FormsPal offers risk-free form editing without personal data recording or any sort of sharing. Feel safe knowing that your data is safe with us!