Flu or influenza is a very contagious disease known to virtually everyone because of the speed with which it spreads across the country each year in the cold season. For the average person, influenza is not a dangerous disease; most people without underlying health conditions after catching it would experience only mild symptoms such as fatigue, chills, muscle aches, sore throat, runny nose, etc.
However, for some people, namely infants, small children, older people and people with specific health conditions flu may pose a serious threat and they can eventually end up with bronchitis, pneumonia, and other complications that bring people into the hospitals or even to ICU. Moreover, CDC reports that thousands of people in the country die from influenza annually.
The good news is that vulnerable groups of people, especially children, can be effectively protected by vaccination. If you want to protect your children and vaccinate them, you will need to fill out and sign a flu shot consent form, this is not a hard task and in this article, you will find everything that you have to know about this form.
To fill flu shot consent form, you just have to follow this short instruction.
Step 1
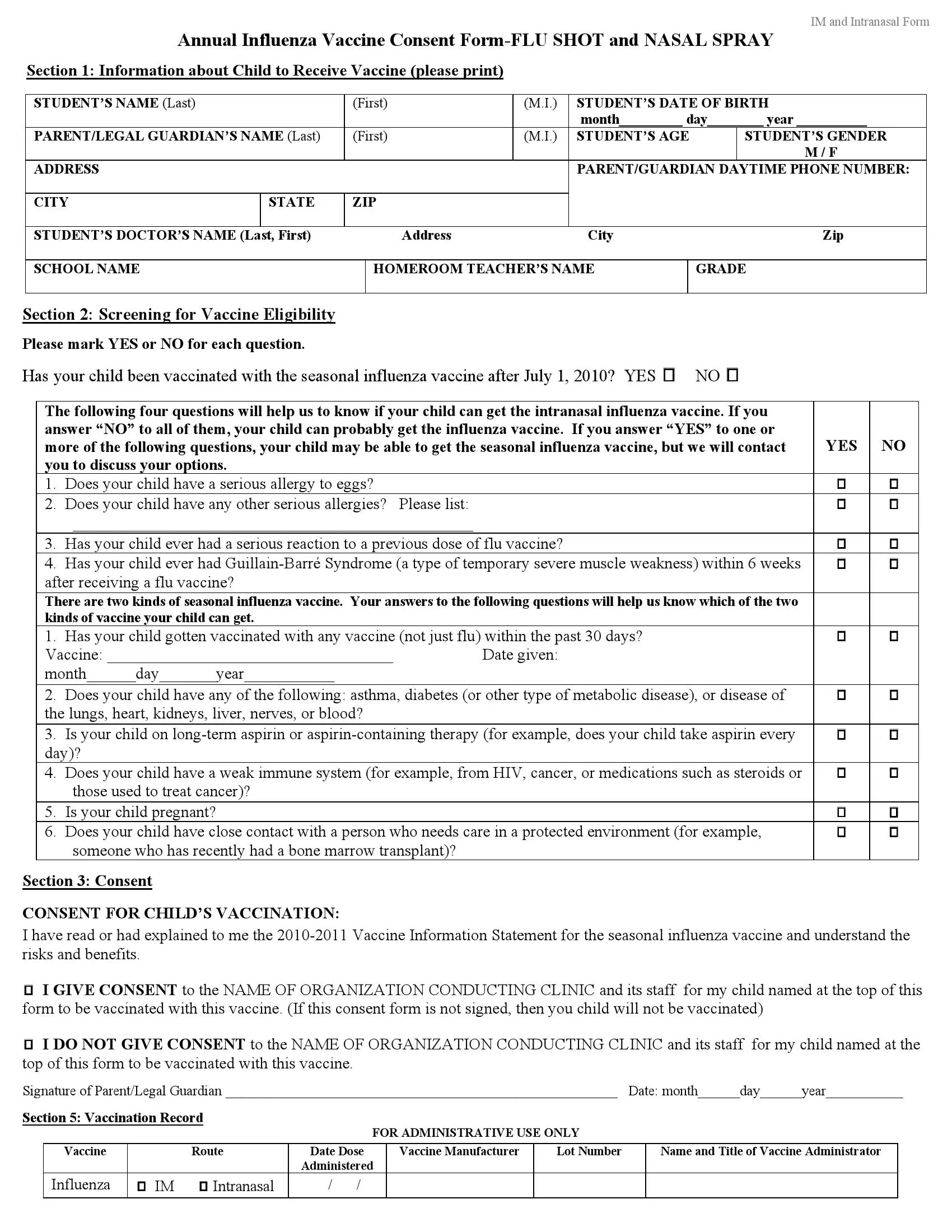
In the first section of the form, you have to write down the personal information of the child that is about to be vaccinated. The information needed is pretty usual:
Step 2
The second section of the form is very important because here, you can find the questions that can reveal that a child is not eligible for vaccination. The questions are about the health conditions; for example, you will be asked whether your child ever had an adverse reaction to any vaccine or whether he or she had GBS. Also, there is a question about a child’s pregnancy, so it is better to talk to them before the vaccination.
Step 3
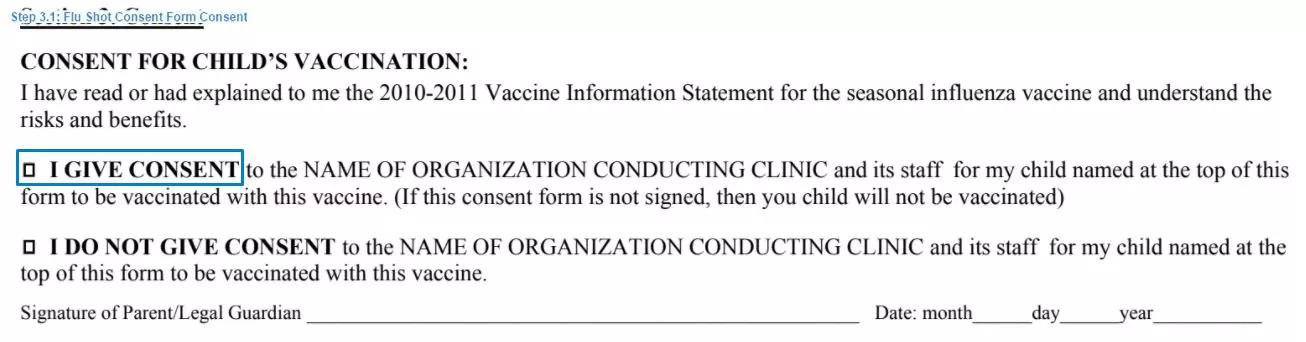
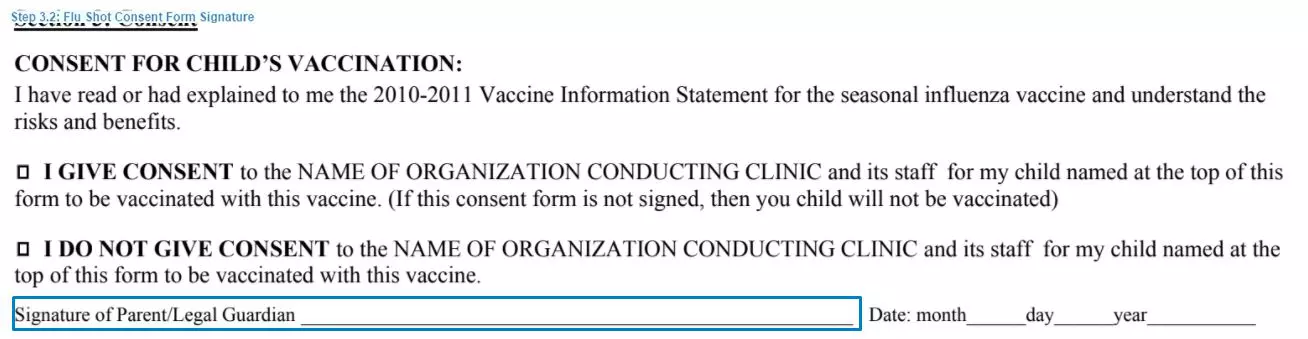
During the third step, you would be able to finally give consent for vaccination. In order to do so, you are required to mark a box next to the text “I give consent” and put your signature and the date in a special place below.
Also, there is one more section in this form, but it is only for administrative use only, so you should not write anything there.
While it is proven that vaccination is the safe and effective way of protecting a child against the most severe symptoms of influenza, it can be possible that your child would experience some adverse reaction, so you need to know them in advance in order to be prepared.
The most widespread adverse reactions after a flu vaccine are redness, swelling, and soreness in a place where the shot was injected. Headache and fever may happen after vaccination as well. The most dangerous adverse reaction but at the same time the least common is the possibility of developing Guillain-Barré Syndrome; however, here, we must outline that such an adverse reaction is very rare and that this illness is curable.
Also, do not be afraid that your child may faint immediately after vaccination, this is a common effect, and in most cases, it does not have any consequences.
In addition, it is important to know that the most severe adverse reaction is allergic so it would be wise to check whether your child has some allergies.
If a severe adverse reaction developed after you and your child have already left a vaccination facility you must immediately call 9-1-1 and report to them that patient was recently vaccinated.