
When using the online PDF tool by FormsPal, you are able to fill in or edit 2010 here and now. Our team is committed to making sure you have the ideal experience with our tool by regularly releasing new functions and upgrades. Our tool has become much more helpful as the result of the latest updates! Currently, filling out PDF forms is simpler and faster than before. All it requires is just a few simple steps:
Step 1: Hit the "Get Form" button at the top of this page to get into our editor.
Step 2: This tool offers the ability to customize PDF documents in a range of ways. Transform it by writing your own text, correct what is originally in the file, and include a signature - all within the reach of a few clicks!
So as to complete this PDF form, make certain you enter the information you need in each and every blank:
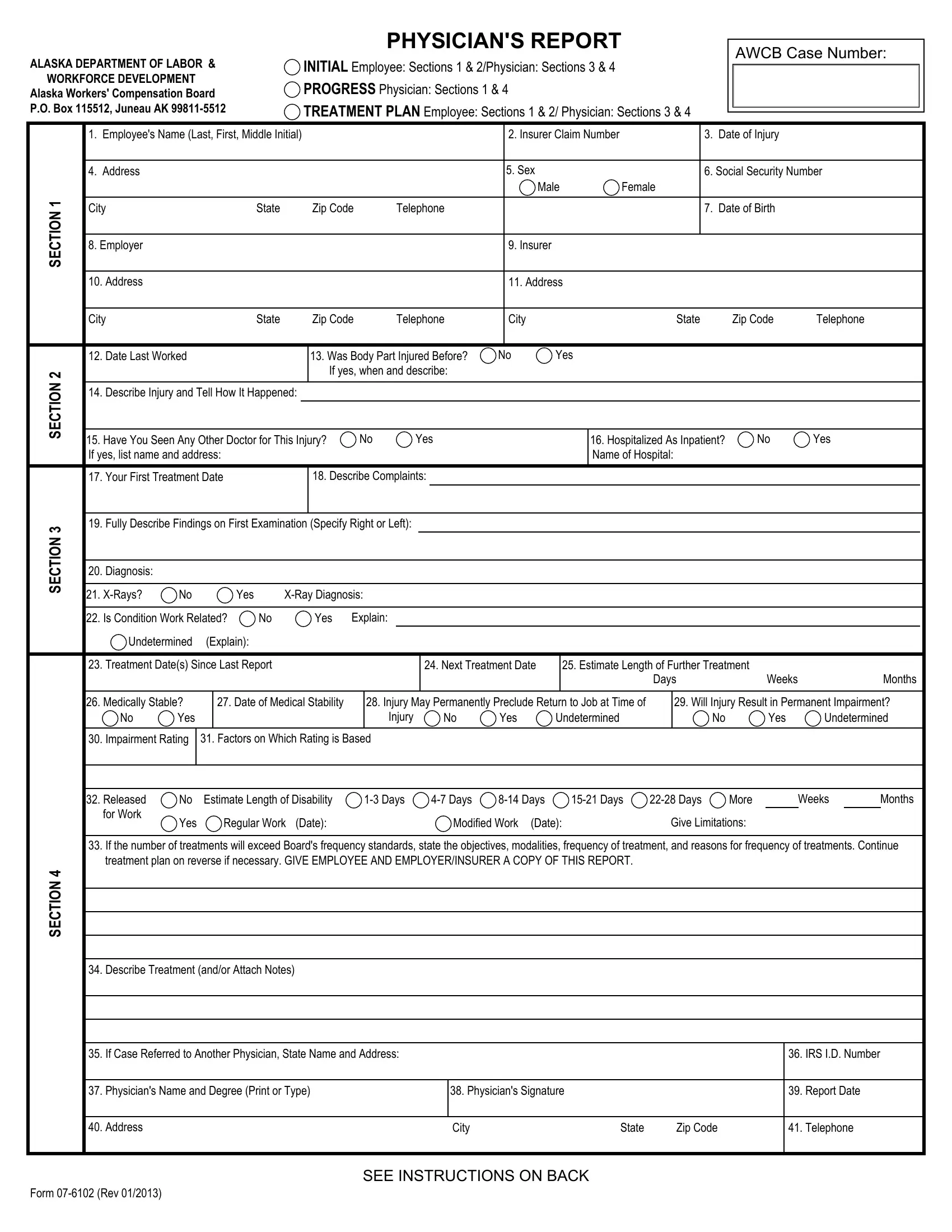
1. Complete the 2010 with a number of major fields. Collect all of the information you need and ensure absolutely nothing is overlooked!
2. Once the previous part is completed, it's time to include the essential specifics in N O T C E S, Fully Describe Findings on First, Diagnosis, XRays, Yes, XRay Diagnosis, Is Condition Work Related, Yes, Explain, Undetermined, Explain, Treatment Dates Since Last Report, Next Treatment Date, Estimate Length of Further, and Days in order to move forward to the 3rd stage.
3. This next segment is considered pretty simple, If Case Referred to Another, Physicians Name and Degree Print, Physicians Signature, IRS ID Number, Report Date, Address, City, State, Zip Code, Telephone, Form Rev, and SEE INSTRUCTIONS ON BACK - every one of these form fields will have to be filled in here.
4. Filling in Employees Name Last First Middle, REMARKS or Treatment Plan, and Report Date is key in this form section - don't forget to don't hurry and be mindful with each and every empty field!
It is possible to get it wrong while filling in the Report Date, consequently you'll want to reread it before you'll finalize the form.
5. The last section to submit this document is critical. You must fill in the necessary blanks, and this includes Medical records in an employees, and Form Rev, before finalizing. Failing to do it might result in an unfinished and possibly nonvalid form!

Step 3: As soon as you have glanced through the information in the blanks, click "Done" to finalize your form. Join FormsPal right now and easily use 2010, all set for downloading. Each and every edit you make is handily kept , which means you can modify the document further as required. Here at FormsPal, we do everything we can to be sure that all of your details are maintained private.