
Using the online PDF editor by FormsPal, you'll be able to complete or alter Form 07 6150 here. Our tool is continually evolving to provide the best user experience possible, and that is due to our dedication to continuous improvement and listening closely to comments from customers. Here's what you'll want to do to start:
Step 1: Press the "Get Form" button at the top of this page to open our PDF editor.
Step 2: This editor will give you the opportunity to customize your PDF document in various ways. Transform it by writing personalized text, adjust original content, and add a signature - all when it's needed!
As for the blank fields of this precise PDF, here is what you need to do:
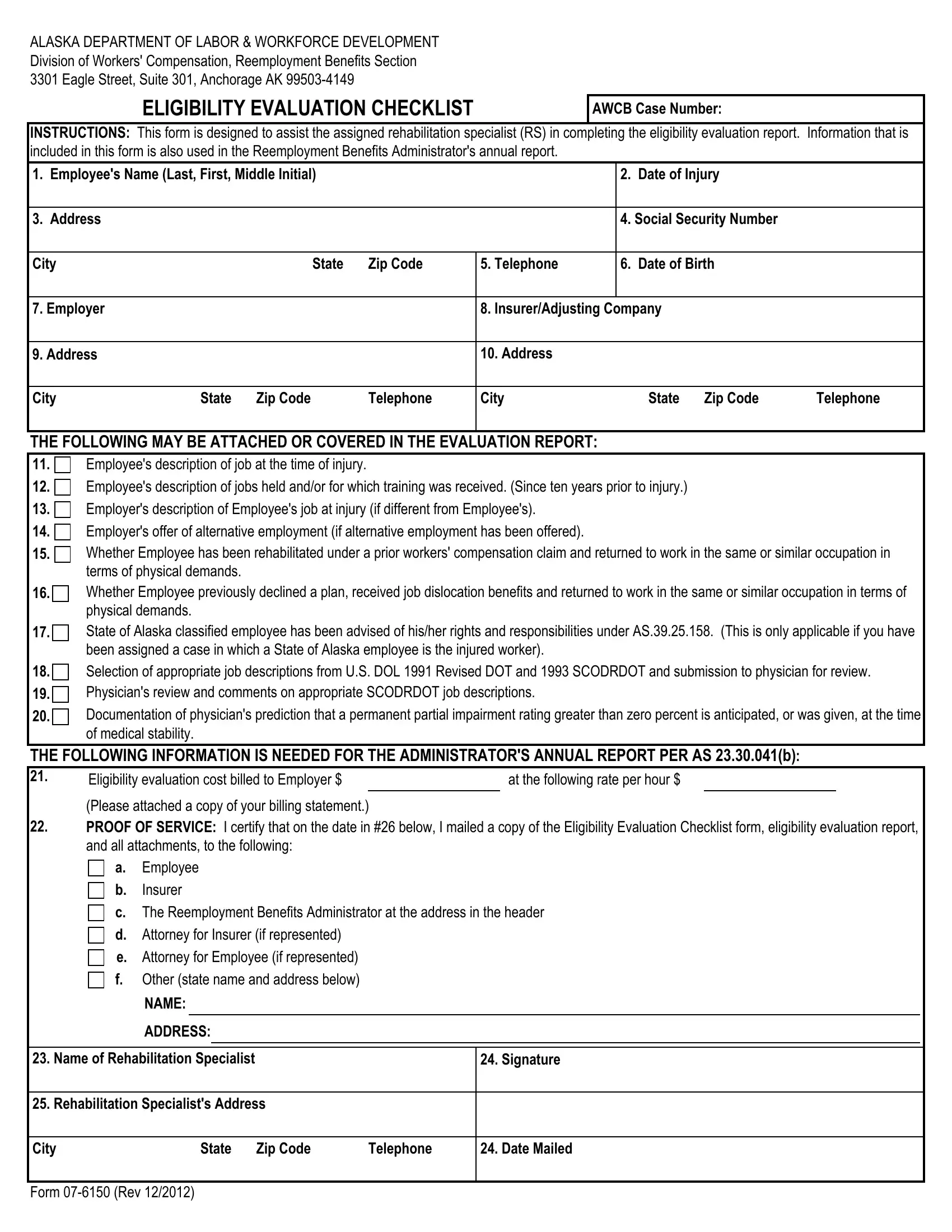
1. The Form 07 6150 usually requires particular details to be inserted. Ensure the subsequent blanks are complete:
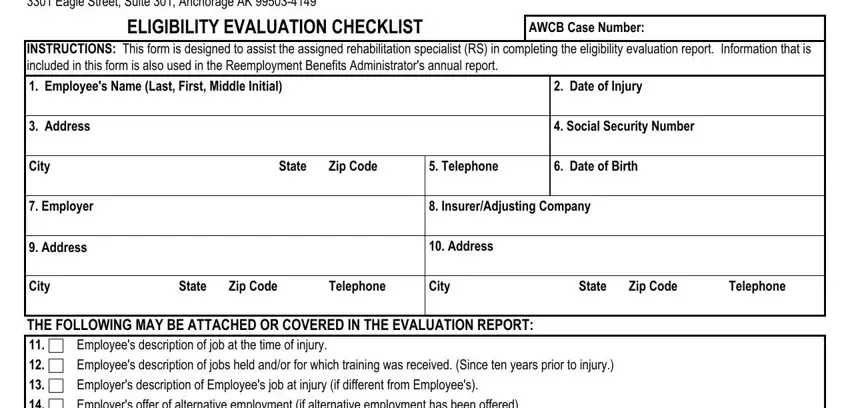
2. Right after this part is done, go on to type in the suitable details in these - Employees description of job at, THE FOLLOWING INFORMATION IS, Eligibility evaluation cost billed, at the following rate per hour, Please attached a copy of your, a Employee, Insurer The Reemployment Benefits, c d Attorney for Insurer if, and NAME.
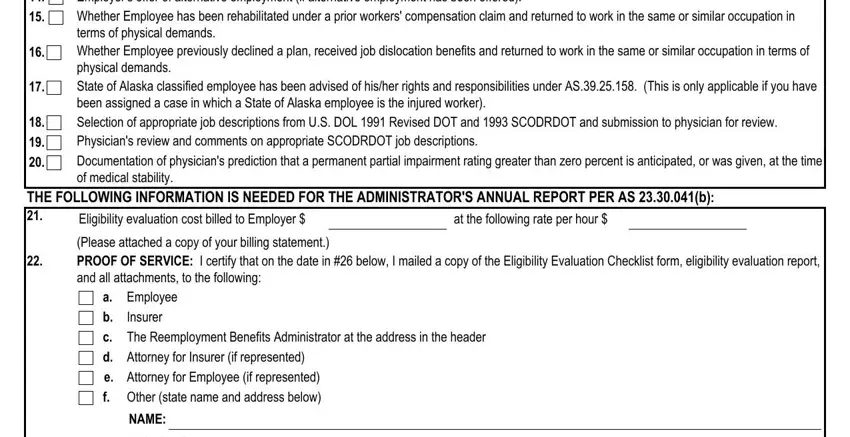
A lot of people frequently make mistakes when filling in Employees description of job at in this part. You should read again what you type in right here.
3. This next portion is mostly about ADDRESS, Name of Rehabilitation Specialist, Signature, Rehabilitation Specialists Address, City, State, Zip Code, Telephone, Date Mailed, and Form Rev - type in every one of these blanks.
Step 3: Prior to moving on, double-check that all form fields were filled in as intended. As soon as you establish that it's good, click on “Done." Grab your Form 07 6150 when you register online for a free trial. Immediately get access to the document inside your FormsPal cabinet, with any edits and changes being all preserved! At FormsPal.com, we aim to guarantee that all your information is kept private.