

Using PDF forms online is a breeze with our PDF tool. You can fill in 1033 form here effortlessly. FormsPal expert team is always working to improve the tool and insure that it is much easier for people with its extensive functions. Take your experience one step further with constantly growing and amazing opportunities available today! It merely requires just a few basic steps:
Step 1: Click on the "Get Form" button at the top of this webpage to get into our PDF editor.
Step 2: This editor lets you modify your PDF in many different ways. Improve it by adding any text, correct original content, and add a signature - all readily available!
With regards to the blank fields of this specific document, here is what you should know:
1. When submitting the 1033 form, make sure to complete all needed blank fields in the associated section. This will help to hasten the work, allowing your information to be processed quickly and appropriately.
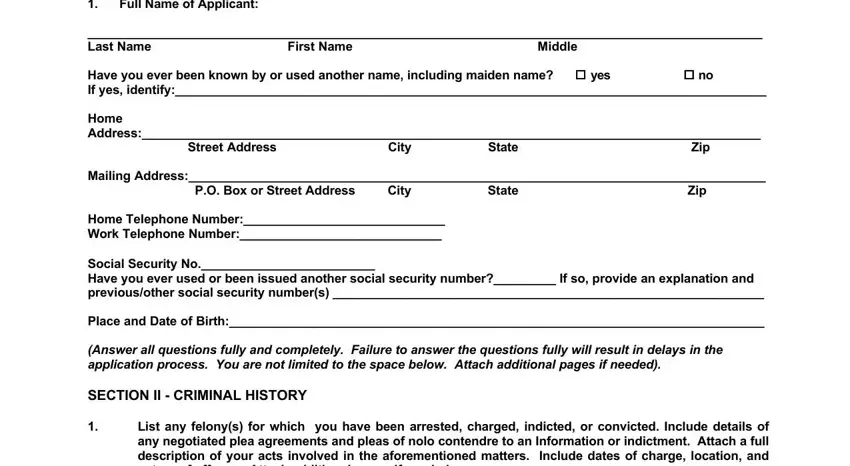
2. Right after performing the previous step, go to the next stage and complete the necessary particulars in these fields - List any felonys for which you, and Provide details of the conviction.
3. Throughout this part, review . Each one of these will need to be completed with greatest accuracy.

Be very mindful while filling out this field and next field, since this is the part where most users make a few mistakes.
4. This fourth paragraph comes next with the next few blank fields to look at: Please specify the name and, and Please describe in detail the.
5. The form has to be finalized with this area. Further one can find an extensive list of fields that need appropriate information to allow your form submission to be complete: relied upon by, the, Insurance Commissioner of, I name of applicant swear under, Signature of Applicant, Date, STATE OF, and COUNTY OF.
Step 3: After going through the form fields you have filled out, press "Done" and you are all set! Join FormsPal today and easily access 1033 form, available for downloading. Every last change made is conveniently kept , which enables you to change the document later on if necessary. FormsPal is focused on the privacy of all our users; we make sure all information coming through our editor stays protected.