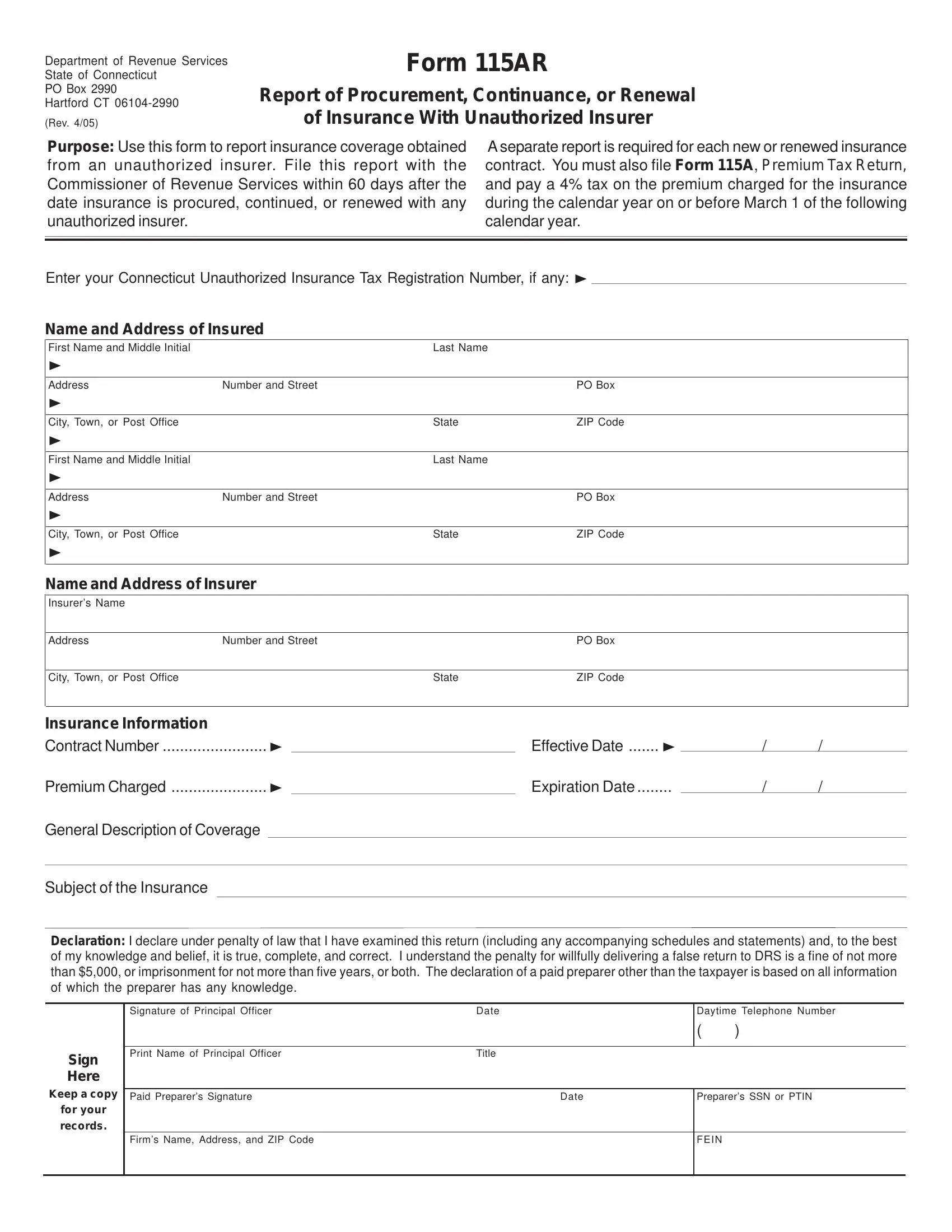
Navigating the complexities of insurance regulations, businesses operating within Connecticut may find themselves wrestling with the specifics of the Form 115AR, a critical document for those engaging with insurance providers outside the state's officially sanctioned list. Essentially, this form serves as a notification to the Commissioner of Revenue Services when insurance is secured, continued, or renewed through what is termed an "unauthorized insurer." This is not just a simple formality; there is a stringent requirement to submit this report within a 60-day window following any such insurance transaction. Moreover, the form is just a piece of the compliance puzzle, as it must be accompanied by Form 115A, the Premium Tax Return, with an accompanying tax of 4% on the premium paid throughout the year to be settled by the upcoming March 1. Each insurance contract demands its report; no bundling of contracts under a single Form 115AR is allowed, underscoring the need for diligent record-keeping by companies. Alongside these obligations, the form captures detailed information about the insured and the insurer, as well as specifics about the insurance contract including the premium, coverage, and the policy’s effective dates. The law enforces accuracy and honesty in these reports, with penalties for falsification that can include fines, imprisonment, or both. By mandating this level of transparency and financial accountability, the State of Connecticut endeavors to safeguard the interests of its business community and ensure that the insurance market operates within the bounds of regulatory oversight.
| Question | Answer |
|---|---|
| Form Name | Form 115Ar |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | SSN, connecticut title 19 form, preparer, 115AR |
Department of Revenue Services
State of Connecticut
PO Box 2990
Hartford CT
(Rev. 4/05)
Form 115AR
Report of Procurement, Continuance, or Renewal
of Insurance With Unauthorized Insurer
Purpose: Use this form to report insurance coverage obtained from an unauthorized insurer. File this report with the Commissioner of Revenue Services within 60 days after the date insurance is procured, continued, or renewed with any unauthorized insurer.
A separate report is required for each new or renewed insurance contract. You must also file Form 115A, Premium Tax Return, and pay a 4% tax on the premium charged for the insurance during the calendar year on or before March 1 of the following calendar year.
Enter your Connecticut Unauthorized Insurance Tax Registration Number, if any:
Name and Address of Insured
First Name and Middle Initial |
|
Last Name |
|
|
|
|
|
|
|
|
|
Address |
Number and Street |
|
PO Box |
|
|
|
|
|
|
|
|
City, Town, or Post Office |
|
State |
ZIP Code |
|
|
|
|
|
|
|
|
First Name and Middle Initial |
|
Last Name |
|
|
|
|
|
|
|
|
|
Address |
Number and Street |
|
PO Box |
|
|
|
|
|
|
|
|
City, Town, or Post Office |
|
State |
ZIP Code |
|
|
|
|
|
|
|
|
Name and Address of Insurer
Insurer’s Name |
|
|
|
|
|
|
|
Address |
Number and Street |
|
PO Box |
|
|
|
|
City, Town, or Post Office |
|
State |
ZIP Code |
|
|
|
|
Insurance Information |
|
|
|
Contract Number ........................ |
Effective Date ....... |
/ |
/ |
Premium Charged ...................... |
Expiration Date |
/ |
/ |
General Description of Coverage |
|
|
|
Subject of the Insurance |
|
|
|
Declaration: I declare under penalty of law that I have examined this return (including any accompanying schedules and statements) and, to the best of my knowledge and belief, it is true, complete, and correct. I understand the penalty for willfully delivering a false return to DRS is a fine of not more than $5,000, or imprisonment for not more than five years, or both. The declaration of a paid preparer other than the taxpayer is based on all information of which the preparer has any knowledge.
Sign
Here
Keep a copy
for your
records.
Signature of Principal Officer |
Date |
Daytime Telephone Number |
|
|
|
( |
) |
|
|
|
|
Print Name of Principal Officer |
Title |
|
|
|
|
|
|
Paid Preparer’s Signature |
Date |
Preparer’s SSN or PTIN |
|
|
|
|
|
Firm’s Name, Address, and ZIP Code |
|
FEIN |
|
|
|
|
|