Navigating the complexities of insurance requirements for Texas Department of Transportation (TxDOT) contracts can feel daunting, yet understanding the TxDOT Form 1560 is fundamental for contractors aiming to comply with state mandates before the initiation of any project. The form serves as a certificate of insurance, verifying that the contractor has obtained the requisite insurance coverages and endorsements as specified by TxDOT. Contractors are tasked with ensuring their insurance agents provide all the necessary details on the form, including types of insurance, policy numbers, coverage limits, and effective dates. The form underscores the need for Workers’ Compensation Insurance, Comprehensive General Liability Insurance, Comprehensive Automobile Liability Insurance, and, if applicable, an Umbrella Policy—each with specific requirements regarding coverage limits and endorsements beneficial to TxDOT. Notably, the certificate must be directly faxed or mailed to the department, offering TxDOT the assurance that contractors are adequately insured, thus safeguarding both parties from potential legal and financial risks involved in transportation projects. This introduction outlines the significance of the form, depicts its role in the preliminary work phase, and delineates the insurance prerequisites it enforces, providing a comprehensive overview vital for contractors engaged in TxDOT projects.
| Question | Answer |
|---|---|
| Form Name | Form 1560 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | txdot form 1560, form 1560, texas department of transportation form 1560, form 1560 cs |

TxDOT Form 1560 (Rev 04/2002) Previous editions of this form may not be used.
Page 1 of 2
Texas Department of Transportation (TxDOT)
CERTIFICATE OF INSURANCE
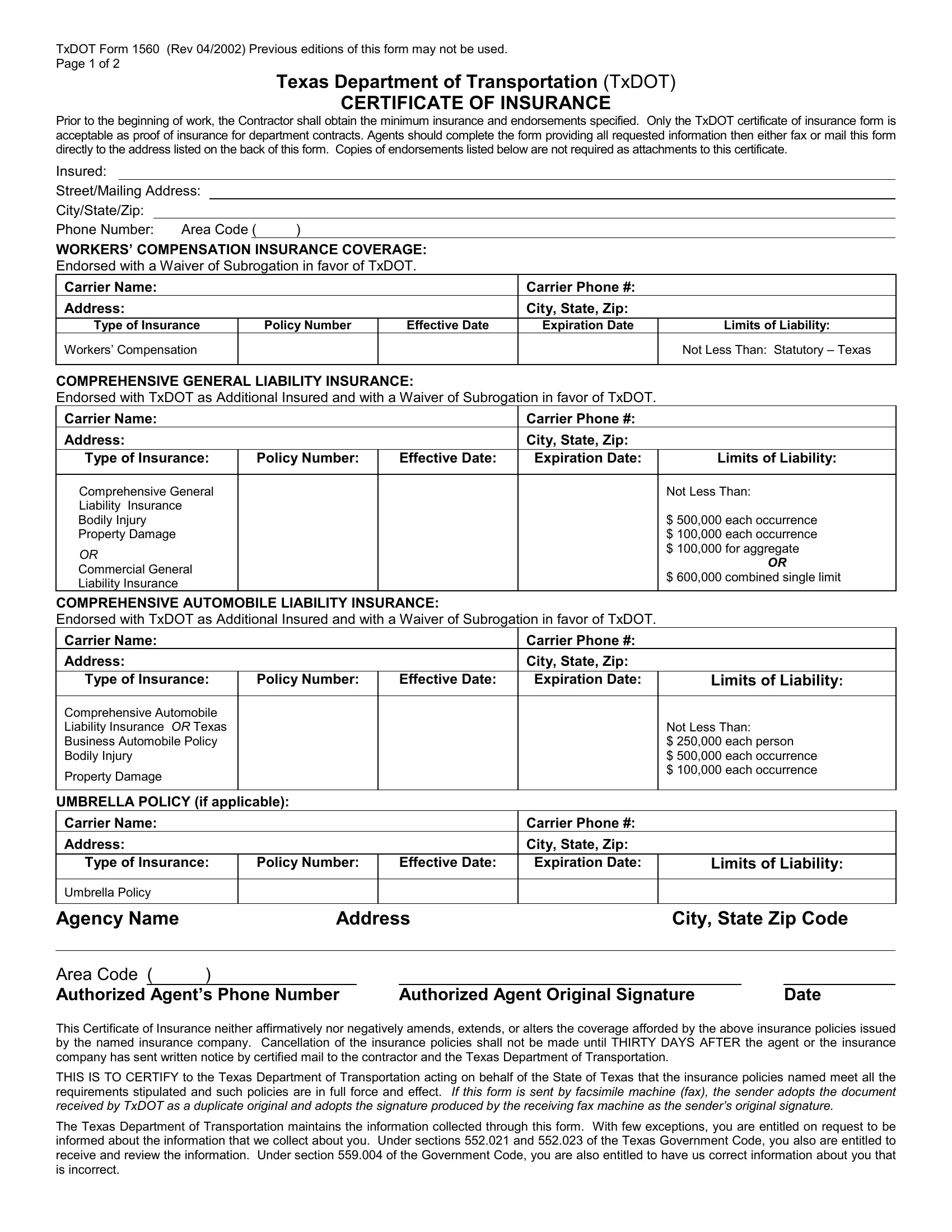
Prior to the beginning of work, the Contractor shall obtain the minimum insurance and endorsements specified. Only the TxDOT certificate of insurance form is acceptable as proof of insurance for department contracts. Agents should complete the form providing all requested information then either fax or mail this form directly to the address listed on the back of this form. Copies of endorsements listed below are not required as attachments to this certificate.
Insured:
Street/Mailing Address:
City/State/Zip:
Phone Number: Area Code ( |
) |
|
|
|
|
||
|
|
|
|
|
|
|
|
WORKERS’ COMPENSATION INSURANCE COVERAGE: |
|
|
|
||||
Endorsed with a Waiver of Subrogation in favor of TxDOT. |
|
|
|
||||
Carrier Name: |
|
|
Carrier Phone #: |
|
|
||
Address: |
|
|
City, State, Zip: |
|
|
||
Type of Insurance |
|
Policy Number |
Effective Date |
Expiration Date |
Limits of Liability: |
|
|
Workers’ Compensation |
|
|
|
|
Not Less Than: Statutory – Texas |
|
|
|
|
|
|
|
|
|
|
COMPREHENSIVE GENERAL LIABILITY INSURANCE:
Endorsed with TxDOT as Additional Insured and with a Waiver of Subrogation in favor of TxDOT.
Carrier Name: |
|
|
|
|
|
Carrier Phone #: |
|
|
|
|
||
Address: |
|
|
|
|
|
City, State, Zip: |
|
|
|
|
||
Type of Insurance: |
Policy Number: |
|
Effective Date: |
Expiration Date: |
|
Limits of Liability: |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||
Comprehensive General |
|
|
|
|
|
Not Less Than: |
|
|||||
Liability Insurance |
|
|
|
|
|
|
|
|
|
|
||
Bodily Injury |
|
|
|
|
|
|
$ 500,000 each occurrence |
|
||||
Property Damage |
|
|
|
|
|
$ 100,000 each occurrence |
|
|||||
OR |
|
|
|
|
|
|
$ 100,000 for aggregate |
|
||||
|
|
|
|
|
|
|
|
OR |
|
|||
Commercial General |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
$ 600,000 combined single limit |
|
||||||
Liability Insurance |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
COMPREHENSIVE AUTOMOBILE LIABILITY INSURANCE: |
|
|
|
|
|
|
||||||
Endorsed with TxDOT as Additional Insured and with a Waiver of Subrogation in favor of TxDOT. |
|
|
|
|
||||||||
Carrier Name: |
|
|
|
|
|
Carrier Phone #: |
|
|
|
|
||
Address: |
|
|
|
|
|
City, State, Zip: |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
Type of Insurance: |
Policy Number: |
|
Effective Date: |
Expiration Date: |
|
Limits of Liability: |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Comprehensive Automobile |
|
|
|
|
|
|
|
|
|
|
||
Liability Insurance |
OR Texas |
|
|
|
|
|
Not Less Than: |
|
||||
Business Automobile Policy |
|
|
|
|
|
$ 250,000 each person |
|
|||||
Bodily Injury |
|
|
|
|
|
|
$ 500,000 each occurrence |
|
||||
Property Damage |
|
|
|
|
|
|
$ 100,000 each occurrence |
|
||||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
UMBRELLA POLICY (if applicable): |
|
|
|
|
|
|
|
|
||||
Carrier Name: |
|
|
|
|
|
Carrier Phone #: |
|
|
|
|
||
Address: |
|
|
|
|
|
City, State, Zip: |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
Type of Insurance: |
Policy Number: |
|
Effective Date: |
Expiration Date: |
|
Limits of Liability: |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Umbrella Policy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Agency Name |
Address |
|
City, State Zip Code |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Area Code ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Authorized Agent’s Phone Number |
|
Authorized Agent Original Signature |
|
|
Date |
|||||||
This Certificate of Insurance neither affirmatively nor negatively amends, extends, or alters the coverage afforded by the above insurance policies issued by the named insurance company. Cancellation of the insurance policies shall not be made until THIRTY DAYS AFTER the agent or the insurance company has sent written notice by certified mail to the contractor and the Texas Department of Transportation.
THIS IS TO CERTIFY to the Texas Department of Transportation acting on behalf of the State of Texas that the insurance policies named meet all the requirements stipulated and such policies are in full force and effect. If this form is sent by facsimile machine (fax), the sender adopts the document received by TxDOT as a duplicate original and adopts the signature produced by the receiving fax machine as the sender’s original signature.
The Texas Department of Transportation maintains the information collected through this form. With few exceptions, you are entitled on request to be informed about the information that we collect about you. Under sections 552.021 and 552.023 of the Texas Government Code, you also are entitled to receive and review the information. Under section 559.004 of the Government Code, you are also entitled to have us correct information about you that is incorrect.
TxDOT Form 1560 (Rev 04/2002)
Page 2 of 2
Texas Department of Transportation
NOTES TO AGENTS:
Agents must provide all requested information then either fax or mail this form directly to the address listed below.
To avoid work suspension, an updated insurance form must reach the address listed below one business day prior to the expiration date. Insurance must be in force in order to perform any work.
Binder numbers are not acceptable for policy numbers.
The certificate of insurance, once on file with the department, is adequate for subsequent department contracts provided adequate coverage is still in effect. Do not refer to specific projects/contracts on this form.
The TxDOT certificate of insurance form is the only acceptable proof of insurance for department contracts.
List the contractor’s legal company name, including the DBA (doing business as) name as the insured or list both the contractor and staff leasing service as insured when a staff leasing service is providing insurance.
This form may be reproduced.
The SIGNATURE of the agent is required. Stamped/typed/printed signatures are not acceptable.
CERTIFICATE OF INSURANCE REQUIREMENTS:
WORKERS’ COMPENSATION INSURANCE:
The contractor is required to have Workers’ Compensation Insurance if the contractor has any employees including relatives.
The word STATUTORY, under limits of liability, means that the insurer would pay benefits allowed under the Texas Workers’ Compensation Law.
GROUP HEALTH or ACCIDENT INSURANCE is not an acceptable substitute for Workers’ Compensation.
COMPREHENSIVE GENERAL LIABILITY INSURANCE or COMMERCIAL GENERAL LIABILITY INSURANCE:
If coverages are specified separately, they must be at least these amounts:
Bodily Injury |
$500,000 each occurrence |
Property Damage |
$100,000 each occurrence |
|
$100,000 for aggregate |
MANUFACTURERS’ or CONTRACTOR LIABILITY INSURANCE is not an acceptable substitute for Comprehensive General Liability Insurance or Commercial General Liability Insurance.
COMPREHENSIVE AUTOMOBILE LIABILITY INSURANCE or TEXAS BUSINESS AUTOMOBILE POLICY:
The coverage amount for a Texas Business Automobile Policy or Comprehensive Automobile Liability may be shown as a minimum of $600,000 Combined Single Limit by a typed or printed entry and deletion of the specific amounts listed for Bodily Injury and Property Damage.
BASIC AUTOMOBILE LIABILITY INSURANCE is not an acceptable substitute for Comprehensive Automobile Liability Insurance or Texas Business Automobile Policy.