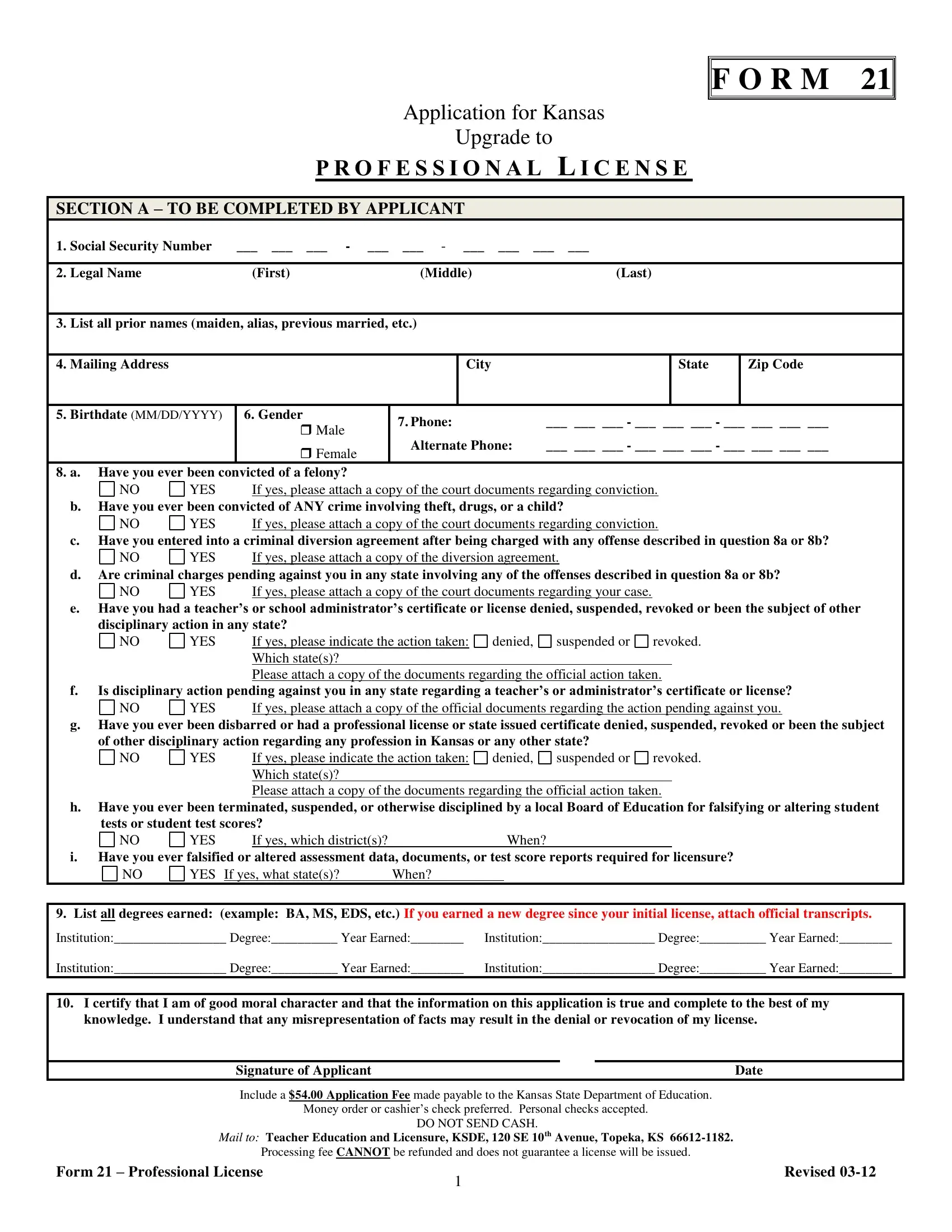
In the state of Kansas, professionals seeking to elevate their qualifications have a structured pathway through the Form 21 application process, aimed at upgrading to a professional license. Integral to this process is the comprehensive gathering of an applicant’s personal and professional details, which includes but is not limited to, social security numbers, legal names—including any previous names—an applicant might have had, mailing addresses, and fundamental demographics such as birthdate and gender. Furthermore, the form delves into questions regarding the applicant's moral and legal standing by inquiring into past convictions, especially those related to felonies, misdemeanors involving theft, drugs, or offenses involving children, and any disciplinary actions against professional certifications or licenses the applicant may have faced. Additionally, the form requests details of the applicant’s educational background, specifically listing all degrees earned, to assess academic qualifications. Another critical component is the verification section, which requires documenting the completion of a district-administered induction and mentoring program—a prerequisite for achieving the professional license. Coupled with a stipulated application fee, the prospects looking to navigate this journey are required to submit the form with accurate and truthful information under the attestation of good moral character, thus embarking on the final steps towards securing a professional license in Kansas.
| Question | Answer |
|---|---|
| Form Name | Form 21 Kansas |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | licensure, Birthdate, YYYY, KSDE |
F O R M 21
Application for Kansas
Upgrade to
P R O F E S S I O N A L L I C E N S E
SECTION A – TO BE COMPLETED BY APPLICANT
1. |
Social Security Number |
___ ___ ___ - ___ |
___ - ___ ___ |
___ ___ |
|
|
|
|
|
|
|
|
|
|
|
2. |
Legal Name |
(First) |
(Middle) |
(Last) |
|
||
|
|
|
|
|
|
|
|
3. |
List all prior names (maiden, alias, previous married, etc.) |
|
|
|
|||
|
|
|
|
|
|
|
|
4. |
Mailing Address |
|
|
City |
|
State |
Zip Code |
|
|
|
|
|
|
|
|
5. |
Birthdate (MM/DD/YYYY) |
6. Gender |
7. Phone: |
___ ___ ___ - ___ ___ ___ - ___ ___ ___ ___ |
|||
|
|
Male |
|||||
|
|
|
|
|
|
|
|
|
|
Female |
Alternate Phone: |
___ ___ ___ - ___ ___ ___ - ___ ___ ___ ___ |
|||
|
|
|
|
|
|
|
|
8. a. Have you ever been convicted of a felony? |
|
|
|
|
|
||
NO
YES |
If yes, please attach a copy of the court documents regarding conviction. |
b.Have you ever been convicted of ANY crime involving theft, drugs, or a child?
NO
YES |
If yes, please attach a copy of the court documents regarding conviction. |
c.Have you entered into a criminal diversion agreement after being charged with any offense described in question 8a or 8b?
NO
YES |
If yes, please attach a copy of the diversion agreement. |
d.Are criminal charges pending against you in any state involving any of the offenses described in question 8a or 8b?
NO |
YES |
If yes, please attach a copy of the court documents regarding your case. |
e.Have you had a teacher’s or school administrator’s certificate or license denied, suspended, revoked or been the subject of other disciplinary action in any state?
NO
YES |
If yes, please indicate the action taken: |
denied,
suspended or
revoked.
Which state(s)?
Please attach a copy of the documents regarding the official action taken.
f.Is disciplinary action pending against you in any state regarding a teacher’s or administrator’s certificate or license?
NO
YES |
If yes, please attach a copy of the official documents regarding the action pending against you. |
g.Have you ever been disbarred or had a professional license or state issued certificate denied, suspended, revoked or been the subject of other disciplinary action regarding any profession in Kansas or any other state?
NO
YES |
If yes, please indicate the action taken: |
denied,
suspended or
revoked.
Which state(s)?
Please attach a copy of the documents regarding the official action taken.
h.Have you ever been terminated, suspended, or otherwise disciplined by a local Board of Education for falsifying or altering student tests or student test scores?
NO
YES |
If yes, which district(s)? |
When? |
i.Have you ever falsified or altered assessment data, documents, or test score reports required for licensure?
NO
YES If yes, what state(s)? |
When? |
|
|
|
|
9. List all degrees earned: (example: BA, MS, EDS, etc.) If you earned a new degree since your initial license, attach official transcripts.
Institution:_________________ Degree:__________ Year Earned:________ |
Institution:_________________ Degree:__________ Year Earned:________ |
Institution:_________________ Degree:__________ Year Earned:________ |
Institution:_________________ Degree:__________ Year Earned:________ |
10.I certify that I am of good moral character and that the information on this application is true and complete to the best of my knowledge. I understand that any misrepresentation of facts may result in the denial or revocation of my license.
Signature of Applicant |
Date |
|
Include a $54.00 Application Fee made payable to the Kansas State Department of Education. |
|
|
|
Money order or cashier’s check preferred. Personal checks accepted. |
|
|
DO NOT SEND CASH. |
|
MAIL TO: Teacher Education and Licensure, KSDE, 120 SE 10th Avenue, Topeka, KS |
|
|
Processing fee CANNOT be refunded and does not guarantee a license will be issued. |
|
|
Form 21 – Professional License |
1 |
Revised |
|
|
|
VERIFICATION OF AN INDUCTION AND MENTORING PROGRAM
Each conditionally or initially licensed teacher, school specialist or school leader must complete a
Mentored Teacher/School Specialist/School Leader information
This form should be completed by the district or building administrator where the mentoring program occurred.
Name (First) |
(Middle) |
(Last) |
|
|
|
Social Security Number ___ |
___ ___ - ___ |
___ - ___ ___ ___ ___ |
OR |
|
|
Teacher identification number from license |
_______________________________________ |
|
If the current school year is the mentor year, do not complete and submit until after May 15th
I verify:
The above named applicant successfully completed a
District Name and Number where mentoring occurred |
Accreditation Information |
NO YES |
||
|
|
State Accredited School? |
||
|
|
If not state accredited, attach verification of accreditation status. |
||
Building Name |
|
|
|
|
|
|
|
|
|
Beginning Date of mentored |
Ending date of mentored |
Assignment of teacher/school specialist/leader |
Grade level |
|
experience (MM/DD/YYYY) |
experience (MM/DD/YYYY) |
during mentored experience |
|
|
|
|
|
|
|
|
|
|
|
|
Administrator’s Name (Please Print or Type)
Administrator’s Position
(May be district or building)
School Phone Number
Administrator’s Signature
Who was the mentor?
Date
_______________________________________________________ |
_________________________________ |
|
Mentor’s Name: |
|
Mentor’s SS# or teacher ID# |
|
|
|
Form 21 – Professional License |
2 |
Revised |
|
|
|
Form 21 – Professional License |
3 |
Revised |
|
|