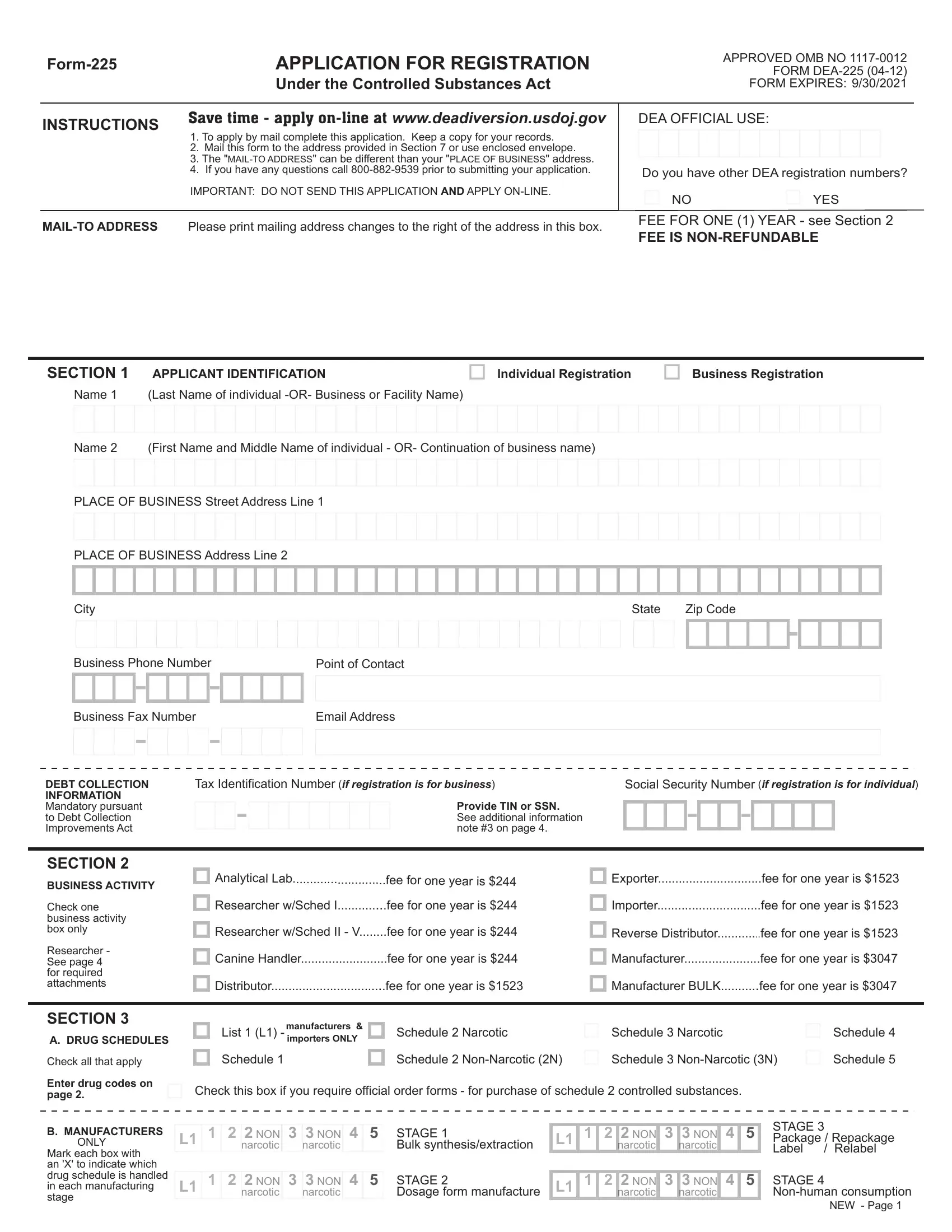
Navigating the complexities of the Controlled Substances Act (CSA) often culminates in the encounter with Form DEA-225, an essential vehicle for entities aiming to lawfully engage with controlled substances. This form serves as a beacon for researchers, manufacturers, distributors, and others by delineating the procedural roadmap for registration under the CSA. The detailed sections of the form intricately lay out the necessities — from applicant identification to business activities, schedules, and drug codes. It mandates specific attention to liability questions, a consequential area given the legal and ethical ramifications tied to controlled substance management. Moreover, the division regarding state licenses underscores the dual necessity of adhering to both federal and state regulatory frameworks — a symbiotic legal relationship often navigated with caution. The financial aspect, as indicated by the non-refundable fees, the option for exemption, and the explicit instruction for selecting a payment method, alongside the solemn declaration required in the applicant’s signature, concretizes the formal engagement with the DEA. The form not only facilitates compliance with regulatory mandates but also embodies the multifaceted considerations spanning legal statutes, ethical considerations, and administrative logistics integral to controlled substance research, distribution, or manufacturing.
| Question | Answer |
|---|---|
| Form Name | Form 225 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | dea, dea 225 form 225 substance, form 225 application, form 225 application control substance |
APPLICATION FOR REGISTRATION |
|
|
Under the Controlled Substances Act |
APPROVED OMB NO
FORM
FORM EXPIRES: 9/30/2021
INSTRUCTIONS |
Save time - apply |
||
1. |
To apply by mail complete this application. Keep a copy for your records. |
||
|
|||
|
2. |
Mail this form to the address provided in Section 7 or use enclosed envelope. |
|
|
3. |
The |
|
|
4. |
If you have any questions call |
|
|
IMPORTANT: DO NOT SEND THIS APPLICATION AND APPLY |
||
|
|
||
Please print mailing address changes to the right of the address in this box. |
|||
DEA OFFICIAL USE:
Do you have other DEA registration numbers?
NO |
YES |
FEE FOR ONE (1) YEAR - see Section 2
FEE IS
SECTION 1 APPLICANT IDENTIFICATION
Individual Registration
Business Registration
Name 1 (Last Name of individual
Name 2 (First Name and Middle Name of individual - OR- Continuation of business name)
PLACE OF BUSINESS Street Address Line 1
PLACE OF BUSINESS Address Line 2
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
State |
Zip Code |
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Business Phone Number |
|
Point of Contact |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Business Fax Number |
|
Email Address |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEBT COLLECTION INFORMATION Mandatory pursuant to Debt Collection Improvements Act
Tax Identification Number (if registration is for business)
Provide TIN or SSN. See additional information note #3 on page 4.
Social Security Number (if registration is for individual)
SECTION 2
BUSINESS ACTIVITY
Check one business activity box only
Researcher - See page 4 for required attachments
Analytical Lab |
fee for one year is $244 |
Researcher w/Sched I |
fee for one year is $244 |
Researcher w/Sched II - V |
fee for one year is $244 |
Canine Handler |
fee for one year is $244 |
Distributor |
fee for one year is $1523 |
Exporter |
fee for one year is $1523 |
Importer |
fee for one year is $1523 |
Reverse Distributor |
fee for one year is $1523 |
Manufacturer |
fee for one year is $3047 |
Manufacturer BULK |
fee for one year is $3047 |
SECTION 3
A. DRUG SCHEDULES
Check all that apply
Enter drug codes on page 2.
manufacturers & |
|
|
Schedule 3 |
Narcotic |
List 1 (L1) importers ONLY |
Schedule 2 |
Narcotic |
||
Schedule 1 |
Schedule 2 |
Schedule 3 |
Check this box if you require official order forms - for purchase of schedule 2 controlled substances.
Schedule 4 Schedule 5
B.MANUFACTURERS ONLY
Mark each box with an 'X' to indicate which drug schedule is handled in each manufacturing stage
L1 1 2 2 NON 3 3 NON 4 5
narcotic narcotic
L1 1 2 2 NON 3 3 NON 4 5
narcotic narcotic
STAGE 1
Bulk synthesis/extraction
STAGE 2
Dosage form manufacture
L1 1 2 2 NON 3 3 NON 4 5
narcotic narcotic
L1 1 2 2 NON 3 3 NON 4 5
narcotic narcotic
STAGE 3
Package / Repackage
Label / Relabel
STAGE 4
NEW - Page 1
SECTION 4
STATE LICENSE(S)
You MUST be currently authorized to prescribe, distribute, dispense, conduct research, or otherwise handle the controlled substances in the schedules for which you are applying under the laws of the state or jurisdiction in which you are operating or propose to operate.
Be sure to include both state license numbers if applicable
State License Number
(REQUIRED)
What state issued this license ?
State Controlled Substance
License Number
(if required)
What state issued this license ?
Expiration |
/ |
/ |
|
Date |
|||
|
|
||
(REQUIRED) |
MM - DD - YYYY |
||
|
|||
Expiration |
/ |
/ |
|
Date |
|||
|
|
||
(if required) |
MM - DD - |
YYYY |
|
SECTION 5
LIABILITY
IMPORTANT
All questions in this section must be answered.
1.Has the applicant ever been convicted of a crime in connection with controlled substance(s) under state or federal law, or been excluded or directed to be excluded from participation in a medicare or state health care program, or is any such action pending?
Date(s) of incident
2.Has the applicant ever surrendered (for cause) or had a federal controlled substance registration revoked, suspended, restricted, or denied, or is any such action pending?
Date(s) of incident
3.Has the applicant ever surrendered (for cause) or had a state professional license or controlled substance registration revoked, suspended, denied, restricted, or placed on probation, or is any such action pending?
YES NO
YES NO
YES NO
Date(s) of incident |
|
|
|
|
|
|
|
|
|
|
|
YES NO |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
4. If the applicant is a corporation (other than a corporation whose stock is owned and traded by the public), association, |
|
|||||||||||
partnership, or pharmacy, has any officer, partner, stockholder, or proprietor been convicted of a crime in connection with |
|
|||||||||||
controlled substance(s) under state or federal law, or ever surrendered, for cause, or had a federal controlled substance |
|
|||||||||||
registration revoked, suspended, restricted, denied, or ever had a state professional license or controlled substance |
|
|||||||||||
registration revoked, suspended, denied, restricted or placed on probation, or is any such action pending? |
|
|||||||||||
Date(s) of incident |
|
|
|
|
|
|
|
|
|
|
Note: If question 4 does not apply to you, be sure to mark 'NO'. |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
It will slow down processing of your application if you leave it blank. |
|
|
|
|
|
|
|
|
|
|
EXPLANATION OF "YES" ANSWERS
Applicants who have answered "YES" to any of the four questions above must provide
a statement to explain each "YES" answer.
Use this space or attach a separate sheet and return with application
Liability question # |
|
Location(s) of incident: |
Nature of incident:
Disposition of incident:
SECTION 6 EXEMPTION FROM APPLICATION FEE
Check this box if the applicant is a federal, state, or local government official or institution. Does not apply to
Business or Facility Name of Fee Exempt Institution. Be sure to enter the address of this exempt institution in Section 1.
The undersigned hereby certifies that the applicant named hereon is a federal, state or local government official or institution, and is exempt from payment of the application fee.
FEE EXEMPT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CERTIFIER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of certifying official (other than applicant) |
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|||||||||||||||||
Provide the name and |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
phone number of the |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Print or type name and title of certifying official |
|
|
|
|
|
|
|
|
|
|
|
|
Telephone No. (required for verification) |
||||||||||||||||||
certifying official |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
SECTION 7 |
Check |
Make check payable to: Drug Enforcement Administration |
|
|
|
|
|
||||||||||||||||||||||||
|
See page 4 of instructions for important information. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
METHOD OF |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mail this form with payment to: |
|
PAYMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
American Express |
|
Discover |
|
Master Card |
Visa |
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
Check one form of |
Credit Card Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
Expiration Date |
|
|
|
DEA Headquarters |
||||||||||||
payment only |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ATTN: Registration Section/ODR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
P.O. Box 2639 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Springfield, VA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sign if paying by |
Signature of Card Holder |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FEE IS |
||||||
credit card |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Printed Name of Card Holder |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
SECTION 8 |
I certify that the foregoing information furnished on this application is true and correct. |
|
|
|
|
|
|||||||||||||||||||||||||
APPLICANT'S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of applicant |
(sign in ink) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Sign in ink
Print or type name and title of applicant
WARNING: 21 USC 843(d), states that any person who knowingly or intentionally furnishes false or fraudulent information in the application is subject to a term of imprisonment of not more than 4 years, and a fine under Title 18 of not more than $250,000, or both.
NEW - Page 3
C. SCHEDULE AND DRUG CODES
Listed below are examples of schedules
For more information, see our website at www.deadiversion.usdoj.gov, 21 CFR 1308, or call
Canine Handler |
must mark schedule 1 |
Distributor |
must mark all schedule 1, drug code 2012 |
Exporter |
must mark all schedule |
Reverse Distributor |
must mark all schedule 1, drug code 2012 |
Importer |
must mark all schedule |
Researcher w/Sched 1 |
must mark schedule 1 |
Manufacturer |
must mark all schedule 1, 2 & List 1 codes |
Researcher w/Sched |
must mark schedule 2 to be manufactured or imported |
|
|
|
as part of research |
If you bulk manufacture a substance, check the 'BULK?' column after the applicable class code.
SCHEDULE 1 NARCOTIC & |
CODE |
BULK? |
|
SCHEDULE 2 NARCOTIC & |
CODE |
BULK? |
|||
|
|||||||||
|
7400 |
|
|
|
Amobarbital (Amytal, Tuinal) |
2125 |
|
||
|
7405 |
|
|
|
Amphetamine (Dexedrine, Adderall) |
1100 |
|
||
|
7395 |
|
|
|
Cocaine (Methyl benzoylecgonine) |
9041 |
|
||
|
1590 |
|
|
|
Codeine (Morphine methyl ester) |
9050 |
|
||
|
Alphacetylmethadol (except LAAM) |
|
9603 |
|
|
|
Dextropropoxyphene (bulk) |
9273 |
|
|
Bufotenine (Mappine) |
|
7433 |
|
|
|
Diphenoxylate |
9170 |
|
|
Marihuana / Cannabidiol |
|
7360 |
|
|
|
Fentanyl (Duragesic) |
9801 |
|
|
Diethyltryptamine (DET) ( |
|
7434 |
|
|
|
Hydrocodone (Dihydrocodeinone) |
9193 |
|
|
Difenoxin 1MG/25UG AtSO4 /DU (Motofen) |
9167 |
|
|
|
Hydromorphone (Diaudid) |
9150 |
|
|
|
Dimethyltryptamine (DMT) |
|
7435 |
|
|
|
9648 |
|
|
|
Etorphine (except HCL) |
|
9056 |
|
|
|
Levorphanol |
9220 |
|
|
Gamma Hydroxybutyric Acid (GHB) |
|
2010 |
|
|
|
Meperidine (Demerol, Mepergan) |
9230 |
|
|
Heroin (Diamorphine) |
|
9200 |
|
|
|
Methadone (Dolophine, Methadose) |
9250 |
|
|
Ibogaine |
|
7260 |
|
|
|
Methamphetamine (Desoxyn) |
1105 |
|
|
Lysergic acid diethylamide (LSD) |
|
7315 |
|
|
|
Methylphenidate (Concerta, Ritalin) |
1724 |
|
|
Mescaline |
|
7381 |
|
|
|
Morphine (MS Contin, Roxanol) |
9300 |
|
|
Marihuana |
|
7360 |
|
|
|
Opium, powdered |
9639 |
|
|
Methaqualone (Quaalude) |
|
2565 |
|
|
|
Oxycodone (Oxycontin, Percocet) |
9143 |
|
|
Normorphine |
|
9313 |
|
|
|
Oxymorphone (Numorphan) |
9652 |
|
|
Peyote |
|
7415 |
|
|
|
Pentobarbital (bulk) (Nembutal) |
2270 |
|
|
Psilocybin |
|
7437 |
|
|
|
Phencyclidine (PCP) |
7471 |
|
|
Tetrahydrocannabinols (THC) |
|
7370 |
|
|
|
Secobarbital (Seconal, Tuinal) |
2315 |
|
SCHEDULE 3 NARCOTIC & |
CODE |
BULK? |
|
SCHEDULE 4 NARCOTIC & |
CODE |
BULK? |
|||
|
Anabolic Steroids |
|
4000 |
|
|
|
Alprazolam (Xanax |
2882 |
|
|
Barbituric acid derivative |
|
2100 |
|
|
|
Barbital (Veronal, Plexonal) |
2145 |
|
|
Benzphetamine (Didrex, Inapetyl) |
|
1228 |
|
|
|
Chloral Hydrate (Noctec) |
2465 |
|
|
Buprenorphine (Buprenex, Temgesic) |
|
9064 |
|
|
|
Chlordiazepoxide (Librium) |
2744 |
|
|
Butabarbital |
|
2100 |
|
|
|
Clonazepam (Klonopin) |
2737 |
|
|
Butalbital |
|
2100 |
|
|
|
Clorazepate (Tranxene) |
2768 |
|
|
Codeine combo product (Empirin) |
|
9804 |
|
|
|
Diazepam (Valium) |
2765 |
|
|
Dihydrocodeine combo product (Compal) |
9807 |
|
|
|
Flurazepam (Dalmane) |
2767 |
|
|
|
Dronabinol in sesame oil soft cap (Marinol) |
7369 |
|
|
|
Lorazepam (Ativan) |
2885 |
|
|
|
2012 |
|
|
|
Meprobamate (Milltown, Equanil) |
2820 |
|
||
|
Hydrocodone combo products (Lorcet, Vicodin) |
9806 |
|
|
|
Midazolam (Versed) |
2884 |
|
|
|
Ketamine (Ketaset, Ketalar) |
|
7285 |
|
|
|
Oxazepam (Serax, |
2835 |
|
|
Morphine combo product |
|
9810 |
|
|
|
Phenobarbital (Fastin, Zantryl) |
2285 |
|
|
Nalorphine (Nalline) |
|
9400 |
|
|
|
Phentermine |
1640 |
|
|
Opium combo product (Paregoric) |
|
9809 |
|
|
|
Temazepam (Restoril) |
2925 |
|
|
Pentobarbital suppository dosage (FP3) |
|
2270 |
|
|
|
Zolpidem (Ambien, Stilnox) |
2783 |
|
|
Phendimetrazine (Plegine, Bontril) |
|
1615 |
|
|
LIST 1 REGULATED CHEMICALS |
CODE |
BULK? |
|
|
Thiopental |
|
2100 |
|
|
** ONLY manufacturers & importers may select List 1 |
|
|
|
|
|
|
|
|
|
|
|
||
SCHEDULE 5 NARCOTIC & |
CODE |
BULK? |
|
|
Ephedrine |
8113 |
|
||
|
Codeine preparations (Robitussin |
9050 |
|
|
|
Phenylpropanolamine |
1225 |
|
|
|
Pyrovalerone (Centroton, Thymergix) |
|
1485 |
|
|
|
Pseudoephedrine |
8112 |
|
WRITE IN ADDITIONAL CODES |
You may write in additional drug codes in this section. Attach a separate sheet if needed. |
|
|
||||||
NEW - Page 2
APPLICATION FOR REGISTRATION |
Supplementary Instructions and Information |
SECTION 1. APPLICANT IDENTIFICATION - Information must be typed or printed in the blocks provided to help reduce data entry errors. A physical address is required in address line 1; a post office box or continuation of address may be entered in address line 2. Fee exempt applicant must list the address of the fee exempt institution. Applicant must enter a valid social security number (SSN), or a tax identification number (TIN) if applying as a business entity.
Debt collection information is mandatory pursuant to the Debt Collection Improvement Act of 1996.
SECTION 2. BUSINESS ACTIVITY - Indicate only one. Each type of business activity requires a separate application. You are required to register as a "manufacturer" if you manufacture a controlled substance or list 1 chemical and then distribute it.
SECTION 3A. SCHEDULES - Applicant should check all schedules to be handled. However, applicant must still comply with state requirements; federal registration does not overrule state restrictions. Check the order form box only if you intend to purchase or to transfer schedule 1 and 2 controlled substances. Order forms will be mailed to the registered address following issuance of a Certificate of Registration.
3B. MANUFACTURER ONLY - Mark the chemical/controlled substance schedule(s) handled in each manufacturing stage listed.
3C. SCHEDULE CODES - Report all chemical/drug codes as required for your business activity. Controlled substances manufacturers and importers must obtain a separate chemical registration if they handle chemicals other than an
SECTION 4. STATE LICENSE(S) - Federal registration by DEA is based upon the applicant's compliance with applicable state and local laws. Applicant should contact the local state licensing authority prior to completing this application. If your state requires a license, provide that number on this application.
SECTION 5. LIABILITY - Applicant must answer all four questions for the application to be accepted for processing. If you answer "Yes" to a question, provide an explanation in the space provided. If you answer "Yes" to several questions, then you must provide a separate explanation describing the date, location, nature, and result of each incident. If additional space is required, you may attach a separate page.
SECTION 6. EXEMPTION - Exemption from payment of application fee is limited to federal, state or local government official or institution. The applicant's superior or agency officer must certify exempt status. The signature, authority title, and telephone number of the certifying official (other than the applicant) must be provided. The address of the fee exempt institution must appear in Section 1.
SECTION 7. METHOD OF PAYMENT - Indicate the desired method of payment. Make checks payable to "Drug Enforcement Administration".
SECTION 8. APPLICANT'S SIGNATURE - Applicant MUST sign in this section or application will be returned. Card holder signature in section 7 does not fulfill this requirement.
ATTACHMENTS: Researcher or canine handler must attach 3 copies of protocol, including curriculum vitae, to conduct research with schedule 1 controlled substances. For clinical investigations, researcher must first submit to FDA a "Notice of Claimed Investigational Exemption for New Drug (IND)". See DEA web site or CFR 1301.18 for details.
NOTICE TO REGISTRANTS MAKING PAYMENT BY CHECK
Authorization to Convert Your Check: If you send us a check to make your payment, your check will be converted into an electronic fund transfer. "Electronic fund transfer" is the term used to refer to the process in which we electronically instruct your financial institution to transfer funds from your account to our account, rather than processing your check. By sending your completed, signed check to us, you authorize us to copy your check and to use the account information from your check to make an electronic fund transfer from your account for the same amount as the check. If the electronic fund transfer cannot be processed for technical reasons, you authorize us to process the copy of your check.
Insufficient Funds: The electronic funds transfer from your account will usually occur within 24 hours, which is faster than a check is normally processed. Therefore, make sure there are sufficient funds available in your checking account when you send us your check. If the electronic funds transfer cannot be completed because of insufficient funds, we may try to make the transfer up to two more times.
Transaction Information: The electronic fund transfer from your account will be on the account statement you receive from your financial institution. However, the transfer may be in a different place on your statement than the place where your checks normally appear. For example, it may appear under "other withdrawals" or "other transactions". You will not receive your original check back from your financial institution. For security reasons, we will destroy your original check, but we will keep a copy of the check for
Your Rights: You should contact your financial institution immediately if you believe that the electronic fund transfer reported on your account statement was not properly authorized or is otherwise incorrect. Consumers have protections under Federal law called the Electronic Fund Transfer Act for an unauthorized or incorrect electronic fund transfer.
ADDITIONAL INFORMATION
No registration will be issued unless a completed application form has been received (21 CFR 1301.13).
In accordance with the Paperwork Reduction Act of 1995, no person is required to respond to a collection of information unless it displays a valid OMB control number. The OMB number for this collection is
The Debt Collection Improvements Act of 1996 (31 U.S.C. §7701) requires that you furnish your Taxpayer Identification Number (TIN) or Social Security Number (SSN) on this application. This number is required for debt collection procedures if your fee is not collectible.
PRIVACY ACT NOTICE: Providing information other than your SSN or TIN is voluntary; however, failure to furnish it will preclude processing of the application. The authorities for collection of this information are §§302 and 303 of the Controlled Substances Act (CSA) (21 U.S.C. §§822 and 823). The principle purpose for which the information will be used is to register applicants pursuant to the CSA. The information may be disclosed to other Federal law enforcement and regulatory agencies for law enforcement and regulatory purposes, State and local law enforcement and regulatory agencies for law enforcement and regulatory purposes, and person registered under the CSA for the purpose of verifying registration. For further guidance regarding how your information may be used or disclosed, and a complete list of the routine uses of this collection, please see the DEA System of Records Notice "Controlled Substances Act Registration Records"
Your Local |
CONTACT INFORMATION |
DEA Office |
All offices are listed on web site |
|
|
|
(800, 877, and 888 are |
INTERNET:
www.deadiversion.usdoj.gov
TELEPHONE:
HQ Call Center (800)
WRITTEN INQUIRIES:
DEA
Attn: Registration Section/ODR
P.O. Box 2639
Springfield, VA
NEW - Page 4