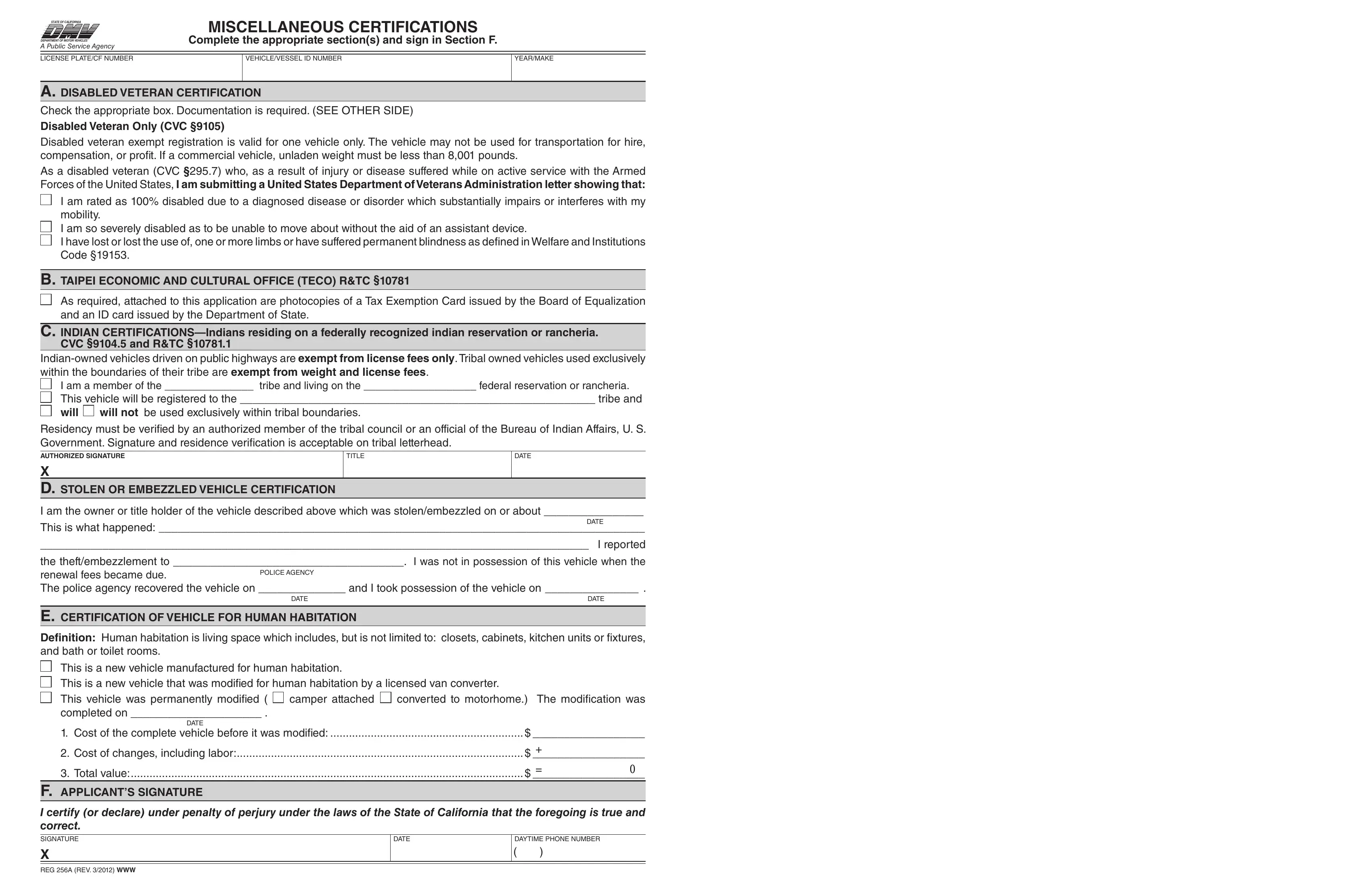
In navigating the complexities of vehicle-related certifications in California, the 256A form serves as a crucial document for a diverse group of applicants, encompassing a wide range of certifications. From disabled veterans seeking exemption from registration fees due to service-connected disabilities, to individuals claiming tax exemptions for vehicles used within tribal boundaries or by the Taipei Economic and Cultural Office, this form ensures compliance with the specific provisions outlined in the California Vehicle Code and other relevant statutes. The form also addresses instances where a vehicle has been stolen or embezzled, outlining the process for owners to certify such incidents to avoid undue fees. Additionally, it caters to the certification of vehicles modified for human habitation, a category that includes vehicles transformed into living spaces through significant modifications. Completing the 256A form accurately is essential for applicants as it requires thorough documentation and adheres to the underpinning legal standards, such as certifying under penalty of perjury the truthfulness of the provided information. Noteworthy is the section dedicated to disabled veterans, which underscores the necessity of a medical statement from the United States Department of Veterans Affairs to qualify for a waiver, hence fostering a streamlined process for those who have served. The form exemplifies the state's commitment to accommodating a variety of specific needs while ensuring each vehicle's registration status aligns with legal requirements.
| Question | Answer |
|---|---|
| Form Name | Form 256A |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | reg 256a form, CVC, 256, in |
STATE OF CALIFORNIA
DEPARTMENT OF MOTOR VEHICLES®
A Public Service Agency
MISCELLANEOUS CERTIFICATIONS
Complete the appropriate section(s) and sign in Section F.
LICENSE PLATE/CF NUMBER
VEHICLE/VESSEL ID NUMBER
YEAR/MAKE
A. DISABLED VETERAN CERTIFICATION
Check the appropriate box. Documentation is required. (SEE OTHER SIDE)
Disabled Veteran Only (CVC §9105)
Disabled veteran exempt registration is valid for one vehicle only. The vehicle may not be used for transportation for hire, compensation, or proit. If a commercial vehicle, unladen weight must be less than 8,001 pounds.
As a disabled veteran (CVC §295.7) who, as a result of injury or disease suffered while on active service with the Armed Forces of the United States, I am submitting a United States Department of Veterans Administration letter showing that:
I am rated as 100% disabled due to a diagnosed disease or disorder which substantially impairs or interferes with my mobility.
I am so severely disabled as to be unable to move about without the aid of an assistant device.
I have lost or lost the use of, one or more limbs or have suffered permanent blindness as deined in Welfare and Institutions Code §19153.
B. TAIpEI ECONOMIC AND CULTURAL OFFICE (TECO) R&TC §10781
As required, attached to this application are photocopies of a Tax Exemption Card issued by the Board of Equalization and an ID card issued by the Department of State.
C. INDIAN
I am a member of the _______________ tribe and living on the ___________________ federal reservation or rancheria.
This vehicle will be registered to the _________________________________________________________ tribe and
will |
will not be used exclusively within tribal boundaries. |
Residency must be veriied by an authorized member of the tribal council or an official of the Bureau of Indian Affairs, U. S. Government. Signature and residence veriication is acceptable on tribal letterhead.
AUTHORIZED SIGNATURE |
TITLE |
DATE |
X
D. STOLEN OR EMBEZZLED VEHICLE CERTIFICATION
I am the owner or title holder of the vehicle described above which was stolen/embezzled on or about ________________
DATE
This is what happened: ______________________________________________________________________________
________________________________________________________________________________________ I reported
the theft/embezzlement to _____________________________________. I was not in possession of this vehicle when the
renewal fees became due.
POLICE AGENCY
The police agency recovered the vehicle on ______________ and I took possession of the vehicle on _______________ .
DATE |
DATE |
|
|
E. CERTIFICATION OF VEHICLE FOR HUMAN HABITATION |
|
Deinition: Human habitation is living space which includes, but is not limited to: closets, cabinets, kitchen units or ixtures, and bath or toilet rooms.
This is a new vehicle manufactured for human habitation. |
|
|
|
This is a new vehicle that was modiied for human habitation by a licensed van converter. |
|
||
This vehicle was permanently modiied ( |
camper attached |
converted to motorhome.) The modiication was |
|
completed on _____________________ . |
|
|
|
DATE |
|
|
|
1. Cost of the complete vehicle before it was modiied: |
$ __________________ |
||
2. Cost of changes, including labor: |
+ |
|
|
$ __________________ |
|||
3. Total value: |
= |
0 |
|
$ __________________ |
|||
F. AppLICANT’S SIGNATURE
I certify (or declare) under penalty of perjury under the laws of the State of California that the foregoing is true and correct.
SIGNATURE
X
REG 256A (REV. 3/2012) WWW
DATE
DAYTIME PHONE NUMBER
()

DOCUMENTATION FOR SECTION A ONLY
VA Regional Ofice Name _____________________________________________
Address _____________________________________________________________
City _______________________________State _______Zip Code ____________
Subject: Medical Statement for
This is to certify that _________________________________________ meets the
(Veteran’s Name)
of a Disabled Veteran, according to the provisions of the California Vehicle Code Section 295.7, as identiied below
(check one or more boxes):
Has a
Is so severely disabled as to be unable to move without the aid of an assistive device; or,
Has lost, or has lost use of, one or more limbs; or,
Has suffered permanent blindness as deined in Section 19153 of the California Welfare and Institutions code.
I certify that I, _______________________________________________ am an authorized employee of the United
(print name)
States Department of Veterans Affairs and I certify under penalty of perjury under the laws of the State of California that the information I have provided is true and correct and that I will retain information suficient to substantiate the certiication and shall make that information available for inspection by the Medical Board of California, at the department’s request. (CVC Section 22511.55). (Note: Assembly Bill 2777, Statutes of 2010, removed the requirement that a physician sign this certiication.)
Executed at (City/State):_________________________________________________ Date:____________________
Signature___________________________________ Printed Name _______________________________________
Phone #:___________________________________
Veteran: Deliver this form to:
1)A local DMV Field Ofice, or
2)By mail to: DMV: Special Processing Unit, MS D238
P.O. Box 932345 Sacramento, CA
REG 256A (REV. 3/2012) WWW