
Should you need to fill out Assister, there's no need to install any sort of applications - just use our PDF editor. To retain our editor on the leading edge of convenience, we strive to adopt user-oriented capabilities and improvements on a regular basis. We are at all times thankful for any feedback - join us in revolutionizing how we work with PDF docs. To begin your journey, consider these easy steps:
Step 1: Click the orange "Get Form" button above. It'll open our pdf editor so you can start filling out your form.
Step 2: This tool enables you to modify PDF forms in a variety of ways. Transform it by adding personalized text, adjust original content, and add a signature - all close at hand!
Completing this PDF demands attention to detail. Make certain all necessary blank fields are filled out properly.
1. Whenever completing the Assister, make certain to incorporate all of the essential blank fields within the associated part. It will help to hasten the work, allowing for your details to be processed promptly and correctly.
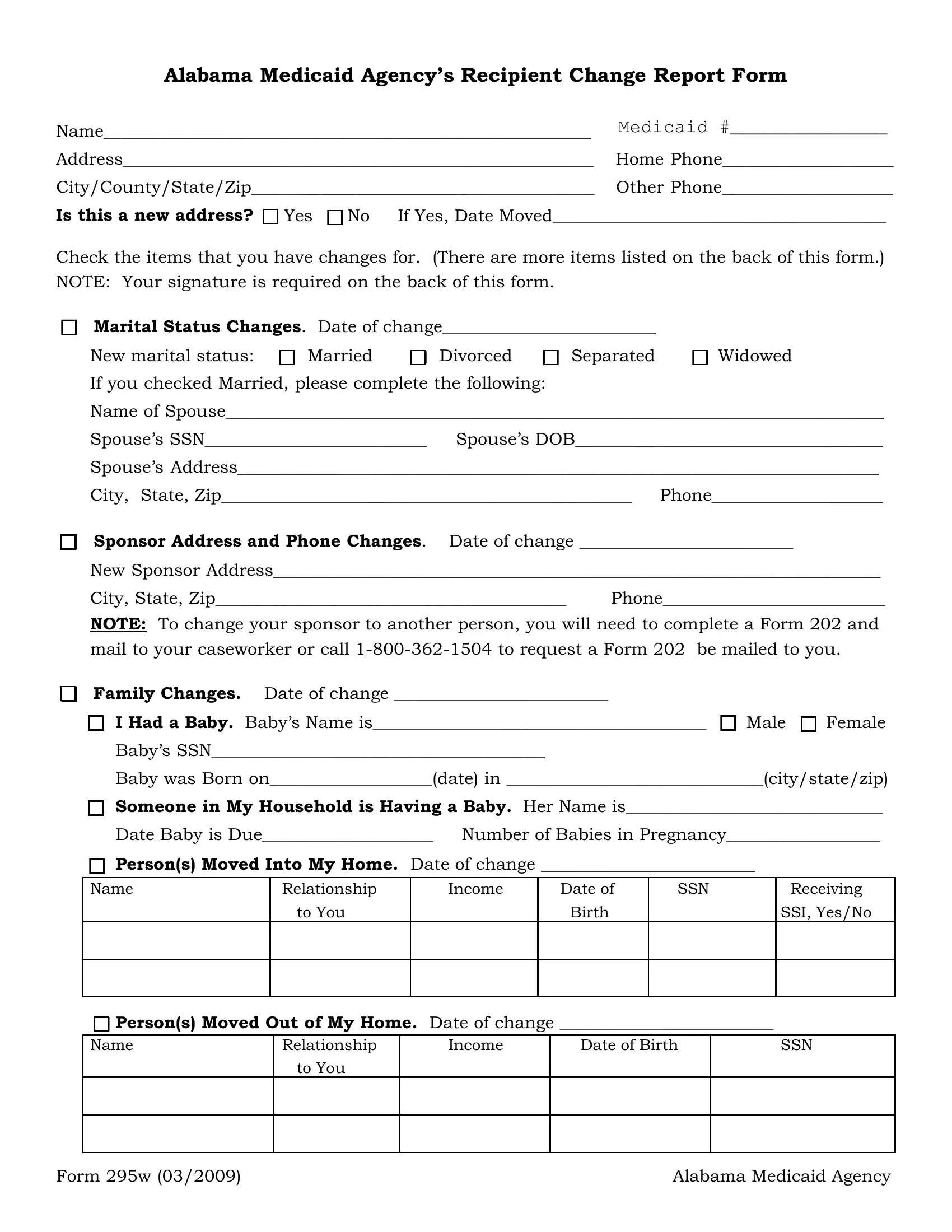
2. Given that the previous array of fields is completed, you need to include the essential specifics in cid Sponsor Address and Phone, New Sponsor Address, City State Zip Phone, NOTE To change your sponsor to, mail to your caseworker or call, cid Family Changes Date of change, cid I Had a Baby Babys Name is cid, Babys SSN, Baby was Born ondate in, cid Someone in My Household is, Date Baby is Due Number of Babies, cid Persons Moved Into My Home, Name, Relationship, and Income so you can progress further.
Be really attentive when filling in cid Family Changes Date of change and Relationship, since this is the part in which most users make errors.
3. This subsequent segment is fairly straightforward, cid Persons Moved Out of My Home, Date of Birth, Relationship, Income, SSN, to You, Form w, and Alabama Medicaid Agency - each one of these blanks will have to be filled in here.
4. This next section requires some additional information. Ensure you complete all the necessary fields - cid Income Changes Date of change, cid New Income, Name Employer Name, Gross Amount Hourly Hours, How, Day, and Address, of Pay before Pay Worked, Often Paid, deductions Rate a Week, Paid, Attach verification of income, cid Loss of Income Person Who No, Date of Last Pay Received, and cid Expense changes Date of change - to proceed further in your process!
5. The form needs to be completed by filling in this area. Here you can find a detailed list of blanks that have to be completed with accurate details to allow your document usage to be faultless: cid Insurance Changes Complete the, located on the Medicaid Website at, cid Report of Death, Name of Recipient Date of death, cid I wish to close my Medicaid, Reason for closing case, cid I wish to withdraw my, cid Other Changes Date of change, Explain, cid By checking this box I declare, and is true and correct.
Step 3: Glance through all the details you've typed into the form fields and click the "Done" button. Grab your Assister the instant you register at FormsPal for a free trial. Conveniently view the pdf document from your personal cabinet, with any edits and changes being all synced! When using FormsPal, you can easily complete forms without the need to be concerned about database leaks or entries getting shared. Our protected software helps to ensure that your private data is maintained safe.