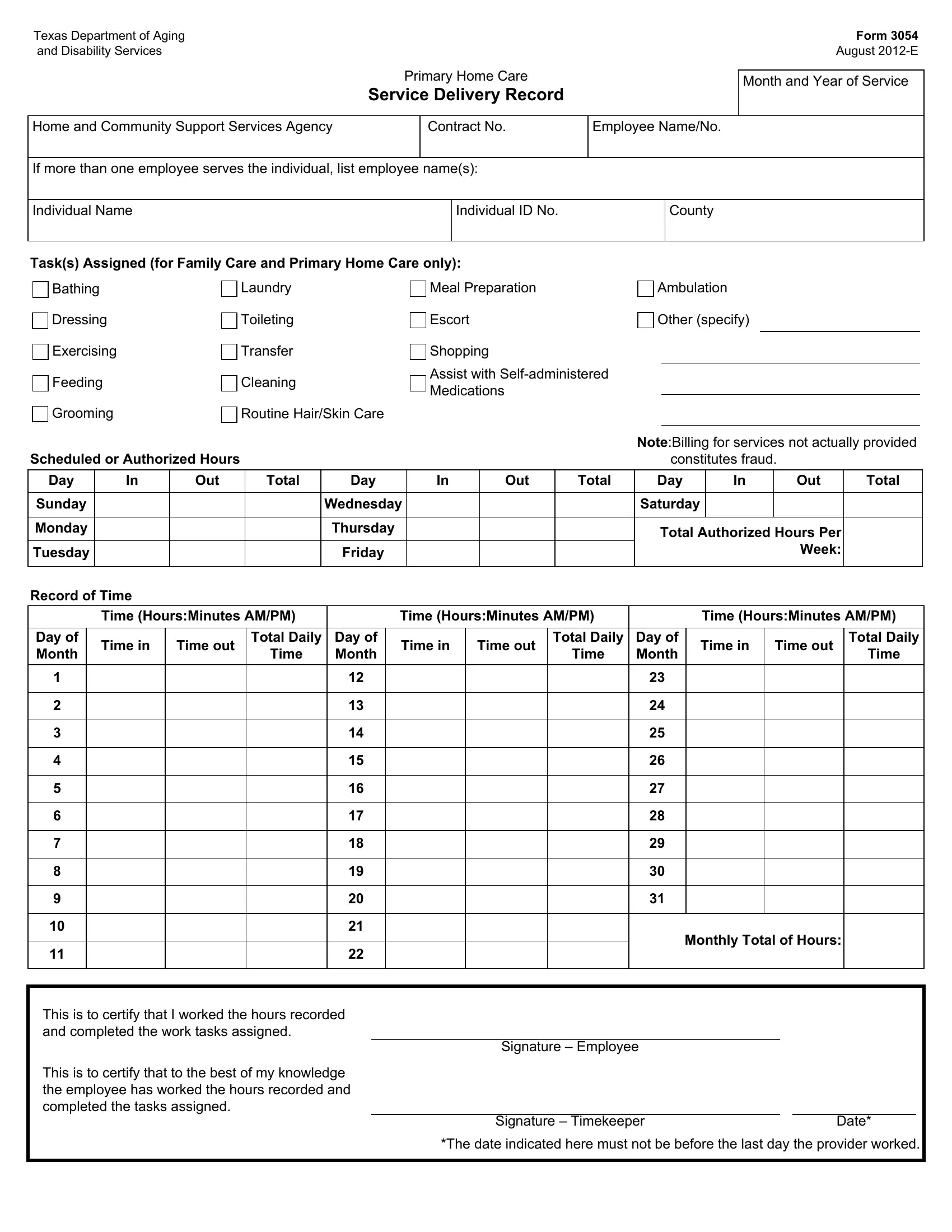
The Texas Department of Aging and Disability Services' Form 3054, also known as the Primary Home Care Service Delivery Record, plays a crucial role in the administration of home and community support services. Issued in August 2012, this form provides a structured method for documenting the services delivered to individuals by Home and Community Support Services Agencies. It encompasses a broad spectrum of personal care tasks stretching from bathing, dressing, and feeding to more specific tasks like grooming, laundry, and even shopping or escort services. Designed to be filled out by employees serving the individual, it asks for detailed entries including employee and individual names, identification numbers, the county, and a list of tasks assigned. Critical to both accountability and billing, the form also includes spaces to record each service occurrence by day, including time in, time out, and total daily hours, aiming to ensure an accurate reflection of the services provided. The form emphasizes the importance of honesty and accuracy in its completion, noting that billing for services not actually provided constitutes fraud. With spaces for signatures from both the employee and a timekeeper, it finalizes the acknowledgement of the work completed according to the schedule or authorized hours, thereby helping to maintain integrity and transparency in home-based care.
| Question | Answer |
|---|---|
| Form Name | Form 3054 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form 3054 dads time sheets 2015, form 3054 dads, texas form 3054, texas department of aging and disability services forms |
Texas Department of Aging
and Disability Services
Primary Home Care
Service Delivery Record
Form 3054
August
Month and Year of Service
Home and Community Support Services Agency
Contract No.
Employee Name/No.
If more than one employee serves the individual, list employee name(s):
Individual Name
Individual ID No.
County
Task(s) Assigned (for Family Care and Primary Home Care only):
Bathing
Dressing
Exercising
Feeding
Grooming
Laundry
Toileting
Transfer
Cleaning
Routine Hair/Skin Care
Meal Preparation
Escort
Shopping
Assist with
Ambulation
Other (specify)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Note:Billing for services not actually provided |
|||||
Scheduled or Authorized Hours |
|
|
|
|
|
|
|
|
|
|
|
|
constitutes fraud. |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Day |
In |
|
Out |
Total |
|
|
Day |
|
In |
|
Out |
|
Total |
|
Day |
|
In |
|
Out |
Total |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Sunday |
|
|
|
|
|
Wednesday |
|
|
|
|
|
|
Saturday |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Monday |
|
|
|
|
|
|
Thursday |
|
|
|
|
|
|
|
Total Authorized Hours Per |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Tuesday |
|
|
|
|
|
|
Friday |
|
|
|
|
|
|
|
|
|
|
|
Week: |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Record of Time |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time (Hours:Minutes AM/PM) |
|
|
|
Time (Hours:Minutes AM/PM) |
|
|
Time (Hours:Minutes AM/PM) |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Day of |
|
Time in |
|
Time out |
Total Daily |
|
Day of |
|
Time in |
Time out |
Total Daily |
|
Day of |
Time in |
|
Time out |
Total Daily |
|||||
Month |
|
|
|
|
Time |
|
Month |
|
|
|
|
|
|
Time |
|
Month |
|
|
|
|
Time |
|
1 |
|
|
|
|
|
|
|
12 |
|
|
|
|
|
|
|
23 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
13 |
|
|
|
|
|
|
|
24 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
14 |
|
|
|
|
|
|
|
25 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
15 |
|
|
|
|
|
|
|
26 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
16 |
|
|
|
|
|
|
|
27 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
17 |
|
|
|
|
|
|
|
28 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
18 |
|
|
|
|
|
|
|
29 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
19 |
|
|
|
|
|
|
|
30 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
|
|
|
|
|
20 |
|
|
|
|
|
|
|
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
21 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Monthly Total of Hours: |
|
|||
11 |
|
|
|
|
|
|
|
22 |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
This is to certify that I worked the hours recorded and completed the work tasks assigned.
Signature – Employee
This is to certify that to the best of my knowledge the employee has worked the hours recorded and
completed the tasks assigned.
Signature – TimekeeperDate*
*The date indicated here must not be before the last day the provider worked.