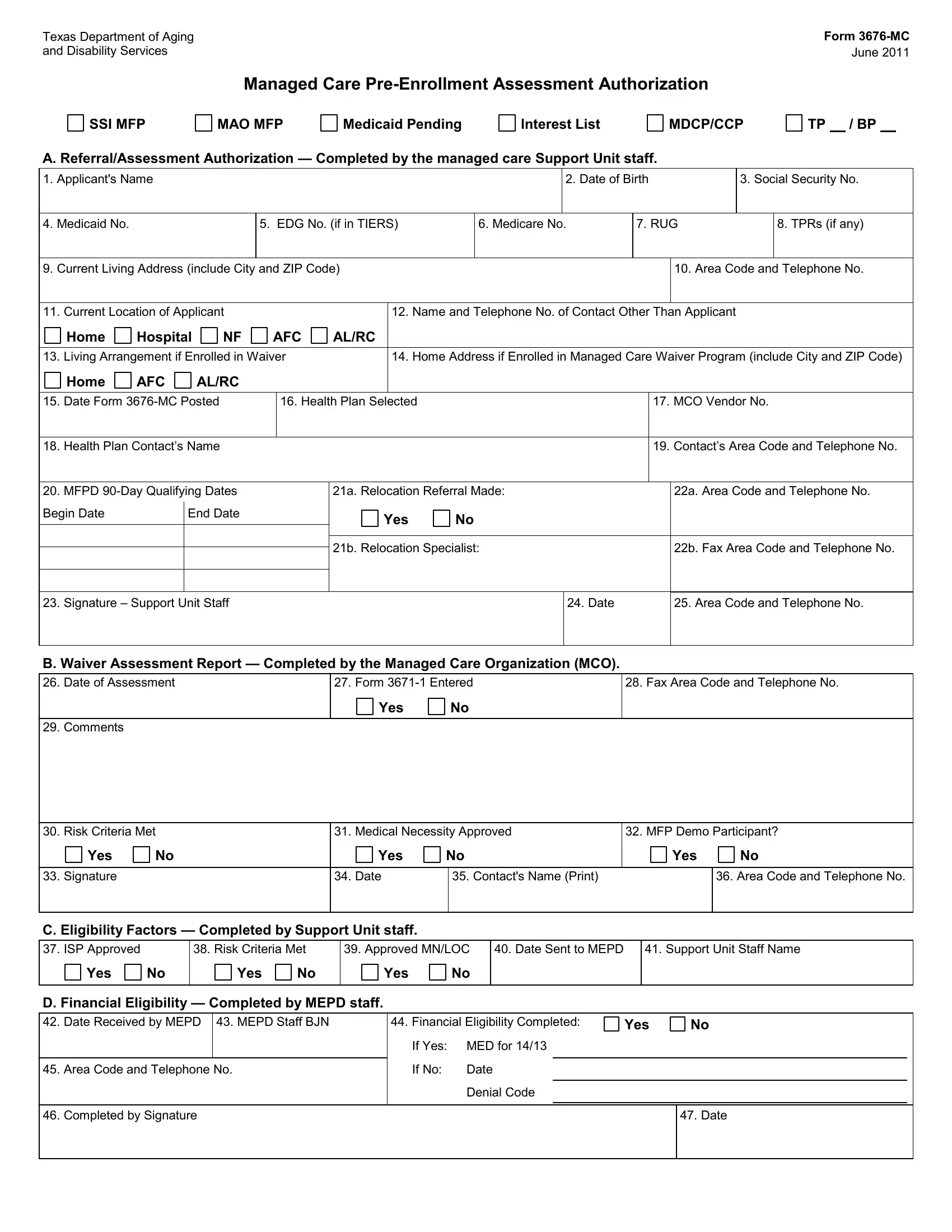
In June 2011, the Texas Department of Aging and Disability Services introduced the 3676-MC form, a crucial document for managing the pre-enrollment assessment process in its managed care programs. This form serves multiple purposes, including authorizing the assessment for enrollment in various managed care programs and assisting individuals who are part of special initiatives such as the Supplemental Security Income (SSI) Program, Money Follows the Person (MFP) Project, and Medicaid for the Aged, Blind, and Disabled (MAO), among others. The form is meticulously divided into several sections, each designed to capture essential information ranging from personal details of the applicant, like their name, date of birth, and social security number, to specific details concerning their current living situation, the health plan selected, and eligibility factors for waiver programs. It also outlines the roles of different stakeholders in the process, including managed care support unit staff, Managed Care Organizations (MCO), and Medicaid Eligibility for Persons with Disabilities (MEPD) staff, ensuring a comprehensive approach to assessing and authorizing managed care pre-enrollment. The detailed structure of the form underlines its significance in streamlining the enrollment process, facilitating effective communication among involved parties, and ensuring individuals receive the appropriate managed care services suited to their needs.
| Question | Answer |
|---|---|
| Form Name | Form 3676 Mc |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 3676-MC, MDCP, hhsc form 1836b printable, form 4214 |
Texas Department of Aging |
Form |
and Disability Services |
June 2011 |
Managed Care
SSI MFP
MAO MFP
Medicaid Pending
Interest List
MDCP/CCP
TP / BP
A. Referral/Assessment Authorization — Completed by the managed care Support Unit staff.
1. |
Applicant's Name |
|
|
|
|
|
|
|
2. Date of Birth |
3. Social Security No. |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
4. |
Medicaid No. |
|
|
5. EDG No. (if in TIERS) |
|
6. Medicare No. |
7. RUG |
|
8. TPRs (if any) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
9. |
Current Living Address (include City and ZIP Code) |
|
|
|
|
|
10. Area Code and Telephone No. |
|||||||||
|
|
|
|
|
|
|
|
|
|
|||||||
11. |
Current Location of Applicant |
|
|
|
12. Name and Telephone No. of Contact Other Than Applicant |
|
|
|||||||||
|
|
Home |
Hospital |
NF |
AFC |
AL/RC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
13. |
Living Arrangement if Enrolled in Waiver |
|
14. Home Address if Enrolled in Managed Care Waiver Program (include City and ZIP Code) |
|||||||||||||
|
|
Home |
AFC |
AL/RC |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
15. |
Date Form |
|
16. Health Plan Selected |
|
|
|
|
17. MCO Vendor No. |
||||||||
|
|
|
|
|
|
|
|
|
|
|||||||
18. Health Plan Contact’s Name |
|
|
|
|
|
|
|
|
19. Contact’s Area Code and Telephone No. |
|||||||
|
|
|
|
|
|
|
|
|||||||||
20. |
MFPD |
|
|
21a. Relocation Referral Made: |
|
|
22a. Area Code and Telephone No. |
|||||||||
Begin Date |
End Date |
|
|
Yes |
No |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
21b. Relocation Specialist:
22b. Fax Area Code and Telephone No.
23. Signature – Support Unit Staff
24. Date
25. Area Code and Telephone No.
B. Waiver Assessment Report — Completed by the Managed Care Organization (MCO).
26. Date of Assessment
27. Form
Yes |
No |
28. Fax Area Code and Telephone No.
29. Comments
30. Risk Criteria Met |
31. Medical Necessity Approved |
32. MFP Demo Participant? |
Yes |
No |
Yes |
No |
Yes |
No |
|
|
|
|
|
|
|
|
33. Signature |
|
34. Date |
|
35. Contact's Name (Print) |
|
36. Area Code and Telephone No. |
|
|
|
|
|
|
|
C. Eligibility Factors — Completed by Support Unit staff.
37.ISP Approved
Yes No
38.Risk Criteria Met
Yes No
39. Approved MN/LOC
Yes |
No |
40. Date Sent to MEPD
41. Support Unit Staff Name
D. Financial Eligibility — Completed by MEPD staff.
42. Date Received by MEPD 43. MEPD Staff BJN
45. Area Code and Telephone No.
44.Financial Eligibility Completed: If Yes: MED for 14/13
If No: Date Denial Code
Yes
No
46. Completed by Signature
47. Date