
Dealing with PDF documents online is always simple with our PDF editor. Anyone can fill out Form 4197 Pec 55555 E 02 10 here without trouble. Our team is relentlessly working to enhance the tool and make it much better for people with its cutting-edge functions. Enjoy an ever-evolving experience today! To get the process started, go through these simple steps:
Step 1: Press the "Get Form" button above. It'll open up our pdf tool so that you could start completing your form.
Step 2: As you launch the tool, you will get the form ready to be filled in. Besides filling out various blanks, you can also perform various other actions with the file, namely putting on custom words, editing the initial text, inserting graphics, placing your signature to the form, and a lot more.
This PDF doc will require specific information; in order to ensure accuracy, you need to heed the guidelines just below:
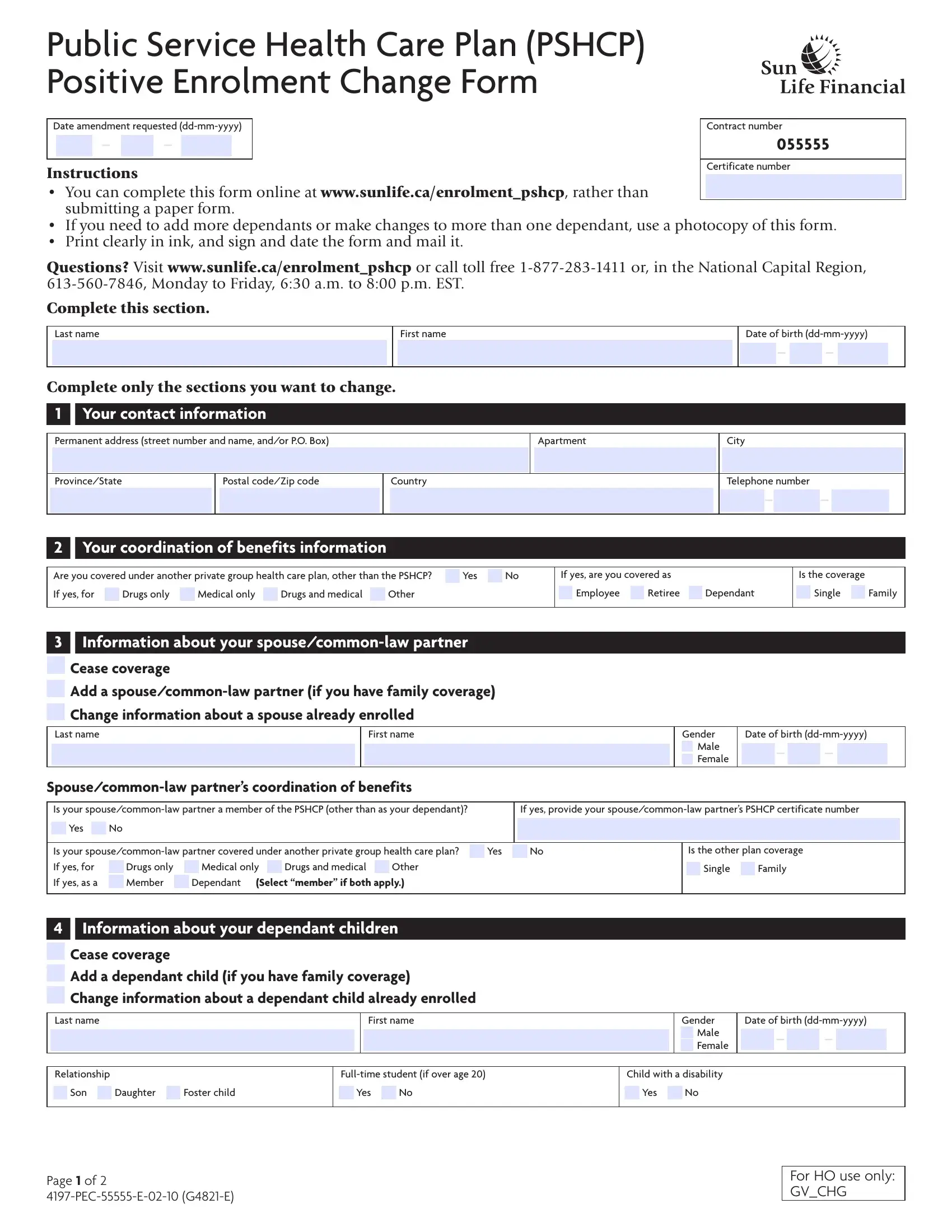
1. Complete the Form 4197 Pec 55555 E 02 10 with a number of essential blanks. Note all of the required information and be sure there's nothing omitted!
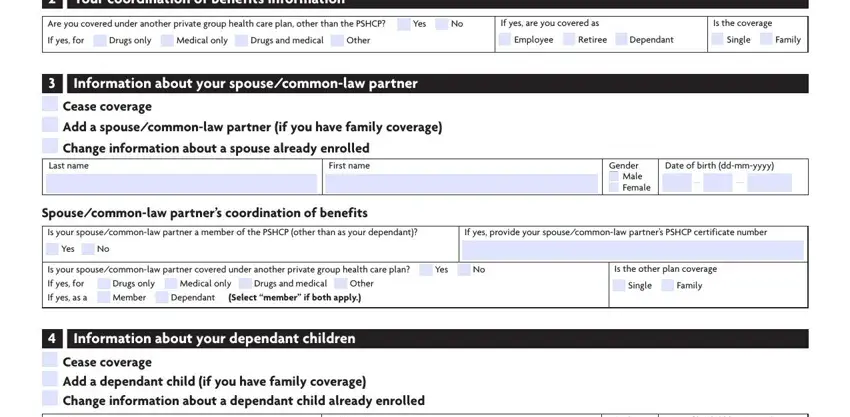
2. When the first part is filled out, go on to type in the relevant details in these: I Your coordination of benefits, Are you covered under another, If yes are you covered as, Is the coverage, If yes for Drugs only Medical, Employee Retiree Dependant, Single Family, I Information about your, Gender Male Female, Date of birth ddmmyyyy, Spousecommonlaw partners, Is your spousecommonlaw partner a, If yes provide your, Yes No, and Is your spousecommonlaw partner.
3. Within this stage, check out I Information about your, First name, Relationship, Fulltime student if over age, Son Daughter Foster child, Yes No, Gender Male Female, Child with a disability, Yes No, Date of birth ddmmyyyy, Page of PECE GE, and For HO use only GVCHG. Every one of these are required to be taken care of with highest accuracy.
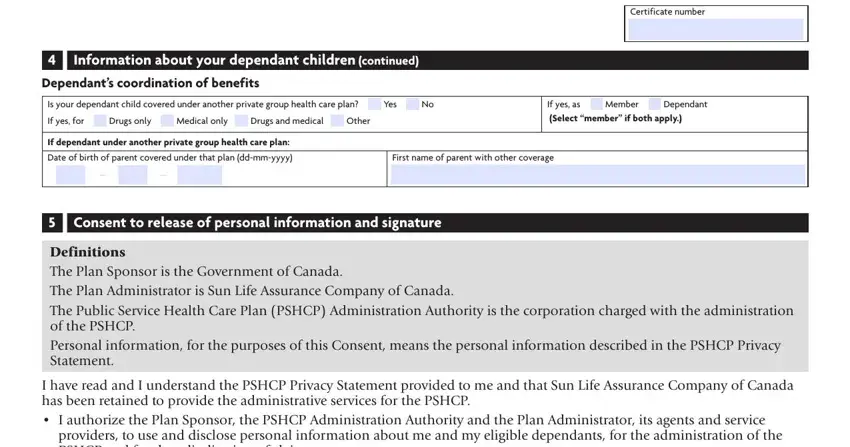
4. This next section requires some additional information. Ensure you complete all the necessary fields - I Information about your, Dependants coordination of benefits, Is your dependant child covered, If yes for Drugs only Medical, If yes as Member Dependant, If dependant under another private, Certificate number, Date of birth of parent covered, First name of parent with other, I Consent to release of personal, Definitions The Plan Sponsor is, I have read and I understand the, and providers to use and disclose - to proceed further in your process!
It's easy to make a mistake when filling out the I Consent to release of personal, for that reason be sure you take another look before you decide to send it in.
5. The pdf must be finalized by dealing with this part. Further you'll see a full set of form fields that need appropriate information for your document usage to be complete: Member signature X, Date ddmmyyyy, Keeping your information, Mailing instructions keep a copy, Mail your completed and signed, Sun Life Financial PSHCP Positive, Page of PECE GE, and For HO use only GVCHG.
Step 3: Just after rereading your fields and details, press "Done" and you are done and dusted! Grab your Form 4197 Pec 55555 E 02 10 once you register at FormsPal for a free trial. Quickly gain access to the pdf file from your FormsPal account page, with any edits and adjustments automatically synced! FormsPal provides protected form editing without personal data recording or sharing. Rest assured that your details are in good hands here!