
Making use of the online editor for PDFs by FormsPal, you are able to complete or modify md form 502b here and now. Our expert team is ceaselessly working to expand the editor and insure that it is even better for users with its handy features. Take full advantage of today's innovative possibilities, and find a trove of unique experiences! To begin your journey, take these simple steps:
Step 1: Press the "Get Form" button at the top of this page to open our tool.
Step 2: As soon as you launch the PDF editor, there'll be the document prepared to be filled out. Apart from filling out different blank fields, you can also perform other actions with the form, such as adding custom words, editing the original textual content, adding graphics, putting your signature on the document, and much more.
As a way to finalize this PDF form, make certain you type in the right information in each area:
1. Whenever filling in the md form 502b, be sure to include all of the needed fields within its relevant form section. This will help speed up the work, allowing for your information to be handled swiftly and properly.
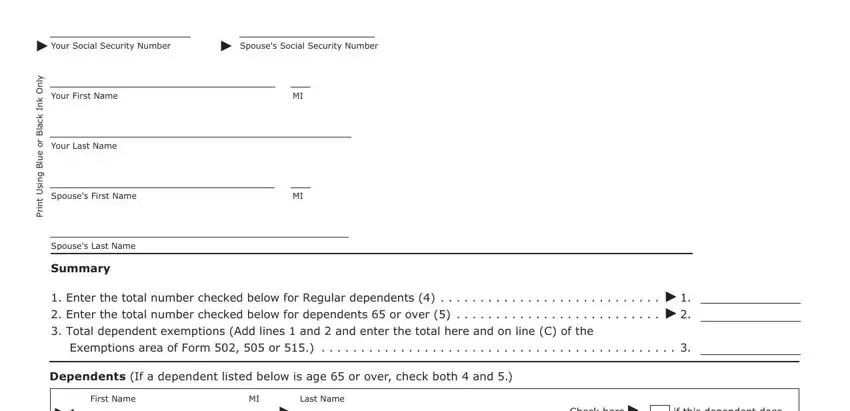
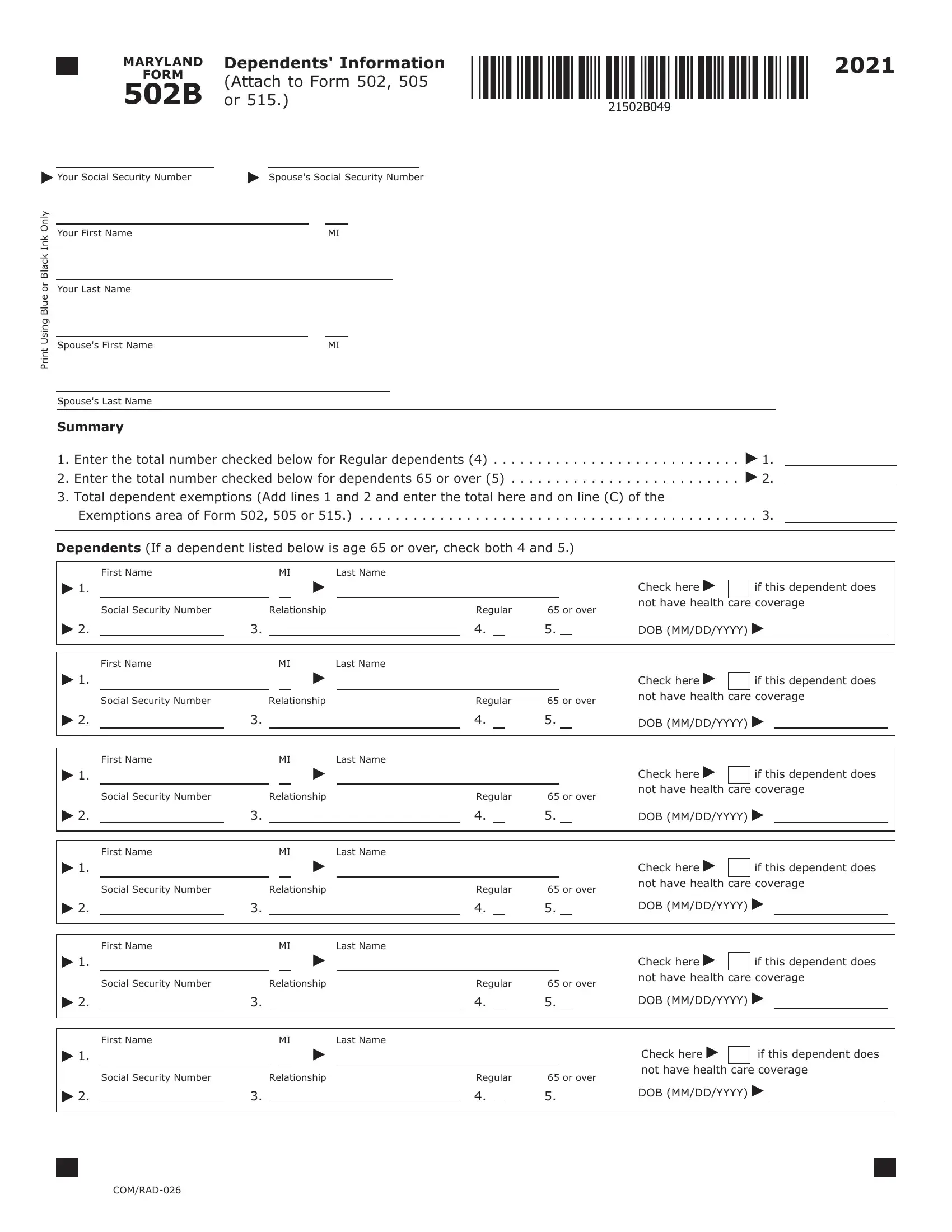
2. After filling out the previous step, head on to the next step and enter the necessary particulars in all these blank fields - Social Security Number, Relationship, Regular, or over, Check here not have health care, DOB MMDDYYYY, First Name, Last Name, Social Security Number, Relationship, Regular, or over, Check here not have health care, if this dependent does, and DOB MMDDYYYY.
3. The following segment will be about Social Security Number, Relationship, Regular, or over, Check here not have health care, if this dependent does, DOB MMDDYYYY, and COMRAD - fill out these blank fields.

4. To move ahead, the following stage requires filling out a handful of blank fields. These include NAME, Dependents Information Attach to, First Name, Last Name, SSN, Social Security Number, Relationship, Regular, or over, First Name, Last Name, Social Security Number, Relationship, Regular, and or over, which are integral to continuing with this particular PDF.
People generally make errors while filling in Last Name in this section. Be certain to reread what you enter here.
5. As a final point, this last subsection is what you will need to complete prior to closing the PDF. The fields at this point are the following: Social Security Number, Relationship, Regular, or over, Check here not have health care, DOB MMDDYYYY, First Name, Last Name, Social Security Number, Relationship, Regular, or over, Check here not have health care, if this dependent does, and DOB MMDDYYYY.
Step 3: Reread the information you have entered into the blanks and then click on the "Done" button. Right after starting a7-day free trial account here, you'll be able to download md form 502b or send it through email right off. The document will also be easily accessible in your personal account page with all your edits. FormsPal ensures your information privacy via a protected system that never saves or shares any private data involved in the process. Feel safe knowing your docs are kept protected every time you use our editor!