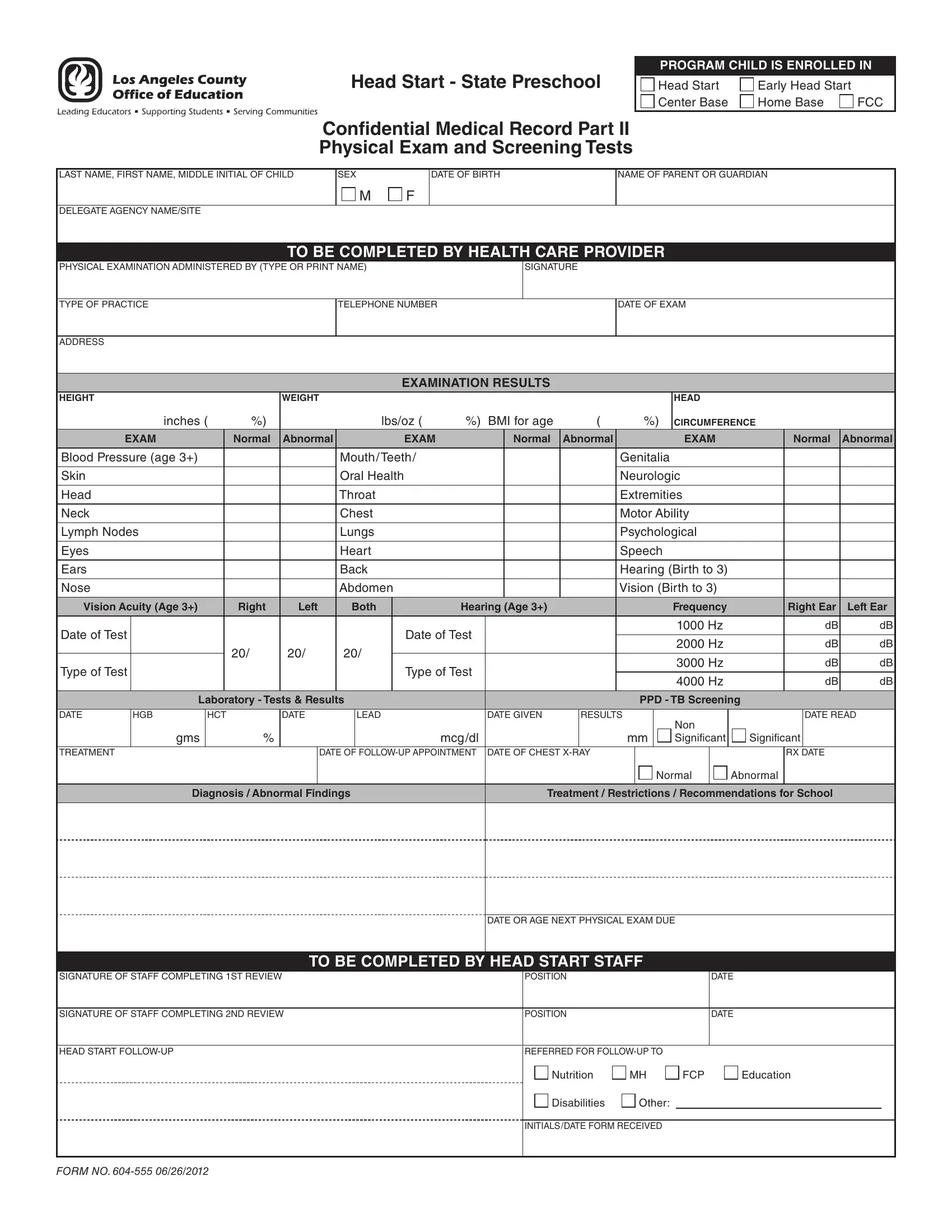
Ensuring the health and well-being of children in early education programs like Head Start and Early Head Start is a fundamental objective, and the Form 604 555 plays a pivotal role in this process. This confidential medical record, designated for children enrolled in these programs, encapsulates a comprehensive physical examination and screening tests outlined in two major parts. The form meticulously captures crucial details starting with basic information about the enrolled child, including name, date of birth, and parental/guardian contact, extending to more detailed health information provided by a health care provider. Physical examinations cover a broad spectrum from height, weight, and body mass index (BMI) assessments to more specific evaluations like blood pressure, oral health, and sensory abilities including hearing and vision. The outcome of these examinations, indicated as normal or abnormal, can profoundly impact a child's engagement in the program, highlighting any immediate need for intervention or ongoing support. The form also delineates follow-up actions, ensuring that children with identified needs receive timely assistance in areas such as nutrition, mental health, and educational support. With an issue date of June 26, 2012, this form embodies a structured approach to monitoring and supporting the health development of children in state preschool programs, ensuring they are physically and psychologically prepared to benefit fully from early educational experiences.
| Question | Answer |
|---|---|
| Form Name | Form 604 555 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | HCT, head start state preschool form 604 555, X-RAY, head start form 604 555 2 |
