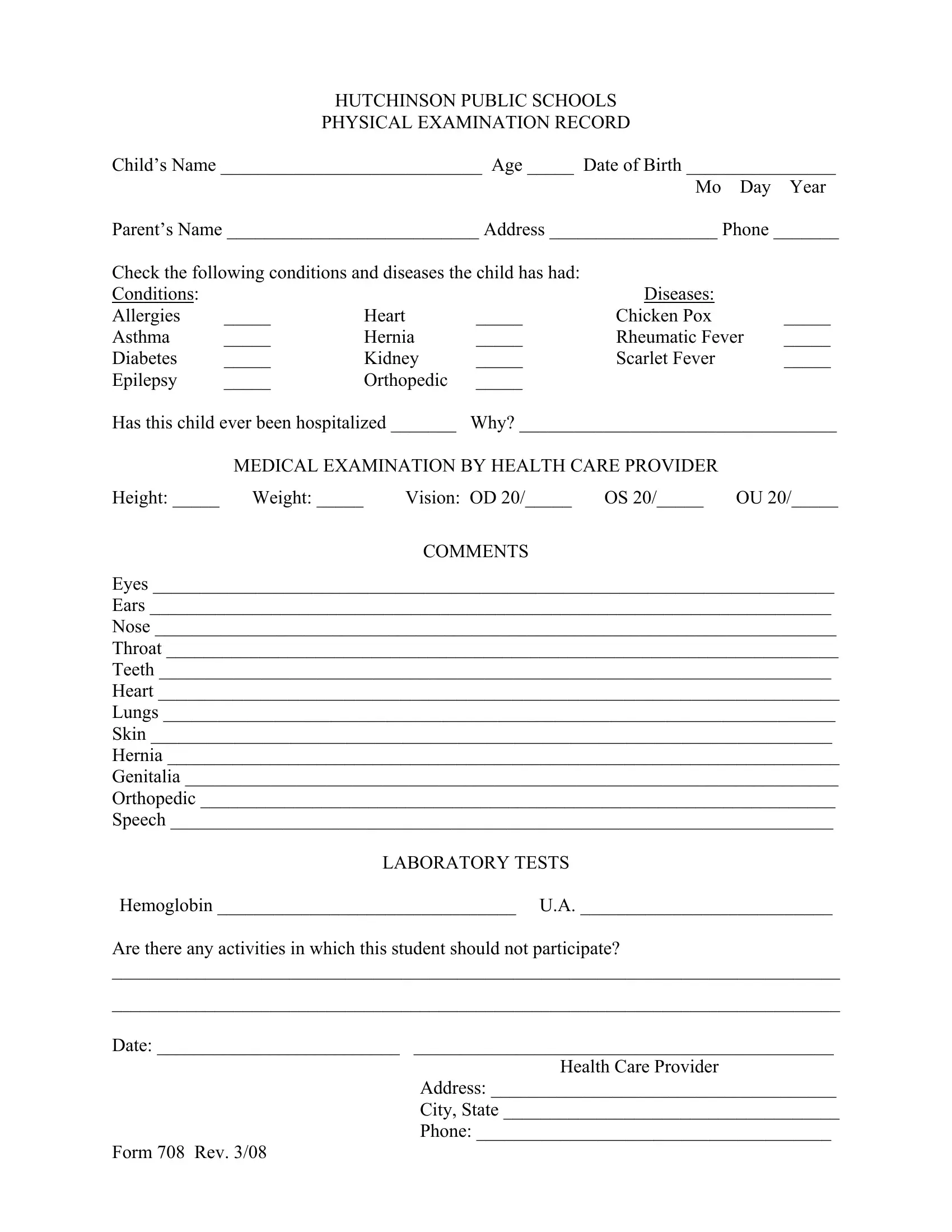
In the educational and healthcare ecosystems, the seamless integration of student health information is pivotal for fostering safe and conducive learning environments. Among the numerous documents that facilitate this, Form 708 holds a significant place. Specifically designed for the Hutchinson Public Schools, this physical examination record serves as a comprehensive conduit for capturing essential health metrics for students. Its scope covers the child’s general information including name, age, and parental contacts, an exhaustive checklist of conditions and diseases such as allergies, asthma, diabetes, to name a few, and even inquiries about any previous hospitalizations. It doesn't stop there. The form further delves into the specifics of the medical examination conducted by a healthcare provider, touching upon vital measurements like height, weight, and vision, as well as detailed inspections of bodily systems — from eyes and ears to heart and lungs. Additionally, it solicits information on any limitations on the student's physical activities, thereby ensuring any health concerns are appropriately accommodated in the school setting. Completed with the healthcare provider's insights and laboratory test results, Form 708 emerges as an essential tool in managing and understanding students' health needs, aiming to bridge the gap between educational aspirations and health prerequisites.
| Question | Answer |
|---|---|
| Form Name | Form 708 |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 15 |
| Avg. time to fill out | 3 min 34 sec |
| Other names | Childs, Genitalia, OU, HUTCHINSON |
