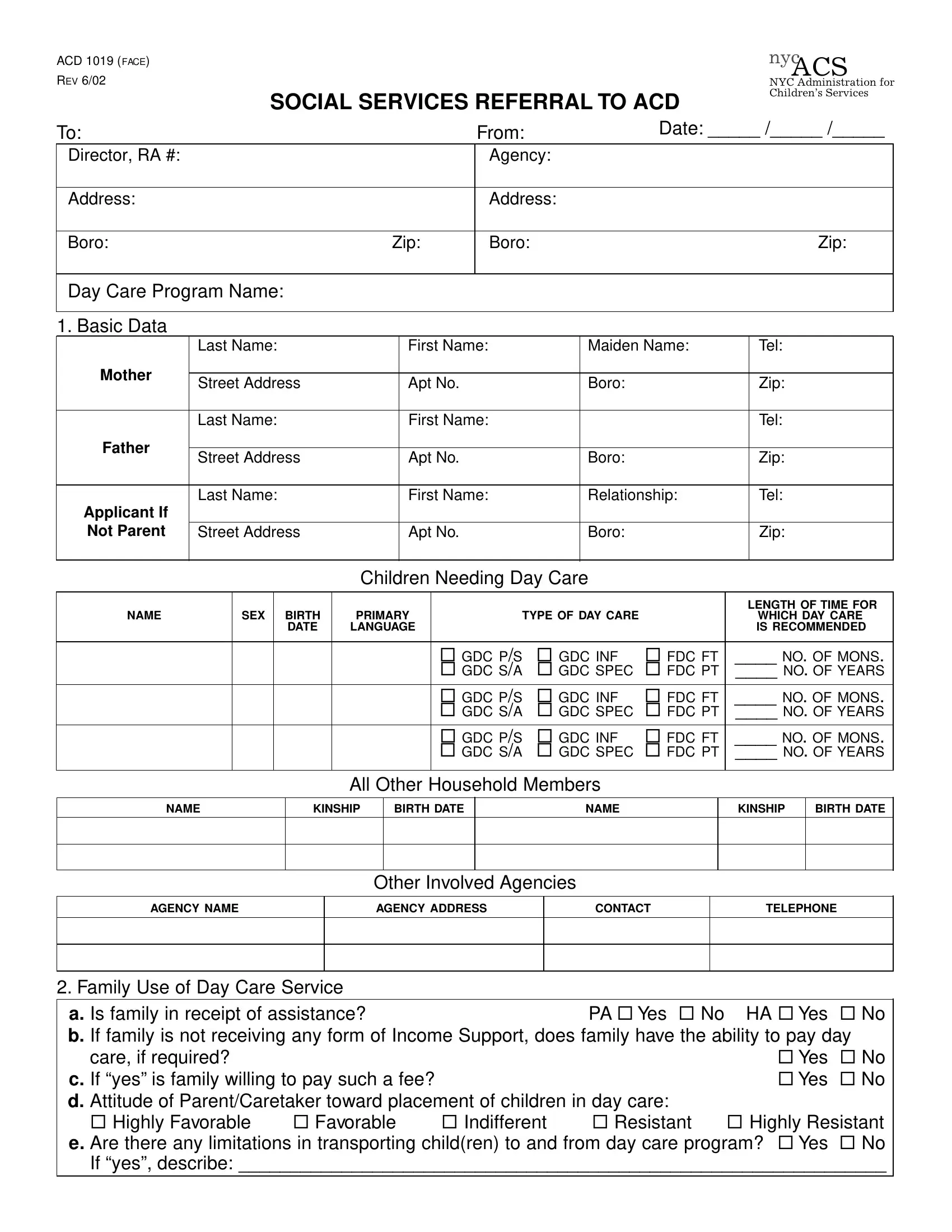
Navigating the complexities of social services can be daunting for families in need of support, making forms like the ACD 1019 essential guides in the process. The ACD 1019 form, revised in June 2002 by the New York City Administration for Children’s Services (ACS), serves as a critical referral document for accessing children’s day care services. It is thoughtfully designed to gather comprehensive data from families seeking day care support, including basic information about the child or children in need, details about the family's circumstances, and the specific type of day care services requested. The form emphasizes the importance of understanding the family's financial situation, their willingness and ability to contribute to day care costs if necessary, and their attitudes towards day care placement. It also provides space for documenting the reason day care is needed, how it will benefit the child or children, and any special considerations for the family that might affect day care placement, such as transportation limitations, physical or emotional health issues, or school-related problems. Through the ACD 1019 form, ACS requires a detailed service plan, encouraging a thorough evaluation of the family's needs and how day care can meet those needs, thereby ensuring that the referral process is both comprehensive and tailored to provide the best possible outcomes for children and their families.
| Question | Answer |
|---|---|
| Form Name | Form Acd 1019 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | KINSHIP, form 1019, GDC, nyc |
ACD 1019 (FACE) |
|
|
|
|
|
|
|
|
|
|
|
nyc |
REV 6/02 |
|
|
|
|
|
|
|
|
|
|
|
ACS |
|
|
|
|
|
|
|
|
|
|
|
NYC Administration for |
|
|
|
SOCIAL SERVICES REFERRAL TO ACD |
|
Children’s Services |
||||||||
|
|
|
|
|||||||||
To: |
|
|
|
|
|
|
From: |
|
|
Date: _____ /_____ /_____ |
||
|
|
|
|
|
|
|
|
|
|
|
||
Director, RA #: |
|
|
|
|
|
|
Agency: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
Address: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Boro: |
|
|
|
Zip: |
|
Boro: |
|
|
|
|
Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Day Care Program Name: |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
1. Basic Data |
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name: |
|
First Name: |
|
Maiden Name: |
|
Tel: |
|||||
Mother |
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
Apt No. |
|
Boro: |
|
|
Zip: |
|||||
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name: |
|
First Name: |
|
|
|
|
Tel: |
||||
Father |
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
Apt No. |
|
Boro: |
|
|
Zip: |
|||||
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name: |
|
First Name: |
|
Relationship: |
|
Tel: |
|||||
Applicant If |
|
|
|
|
|
|
|
|
|
|
|
|
Not Parent |
Street Address |
|
Apt No. |
|
Boro: |
|
|
Zip: |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Children Needing Day Care |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LENGTH OF TIME FOR |
|
NAME |
|
SEX |
BIRTH |
PRIMARY |
|
TYPE OF DAY CARE |
|
|
WHICH DAY CARE |
|||
|
|
|
DATE |
LANGUAGE |
|
|
|
|
|
|
IS RECOMMENDED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
¨ GDC P/S |
¨ GDC INF |
¨ FDC FT |
____ NO. OF MONS. |
|||
|
|
|
|
|
|
¨ GDC S/A |
¨ GDC SPEC |
¨ FDC PT |
____ NO. OF YEARS |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
¨ GDC P/S |
¨ GDC INF |
¨ FDC FT |
____ NO. OF MONS. |
|||
|
|
|
|
|
|
¨ GDC S/A |
¨ GDC SPEC |
¨ FDC PT |
____ NO. OF YEARS |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
¨ GDC P/S |
¨ GDC INF |
¨ FDC FT |
____ NO. OF MONS. |
|||
|
|
|
|
|
|
¨ GDC S/A |
¨ GDC SPEC |
¨ FDC PT |
____ NO. OF YEARS |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
All Other Household Members
NAME |
KINSHIP |
BIRTH DATE |
NAME |
KINSHIP |
BIRTH DATE |
|
|
|
|
|
|
|
|
|
|
|
|
Other Involved Agencies
AGENCY NAME |
AGENCY ADDRESS |
CONTACT |
TELEPHONE |
|
|
|
|
|
|
|
|
|
|
|
|
2. Family Use of Day Care Service
a. Is family in receipt of assistance?PA ¨ Yes ¨ No HA ¨ Yes ¨ No b. If family is not receiving any form of Income Support, does family have the ability to pay day
care, if required? |
|
|
|
¨ Yes |
¨ No |
c. If “yes” is family willing to pay such a fee? |
|
|
¨ Yes |
¨ No |
|
d. Attitude of Parent/Caretaker toward placement of children in day care: |
|
|
|||
¨ Highly Favorable |
¨ Favorable |
¨ Indifferent |
¨ Resistant |
¨ Highly Resistant |
|
e. Are there any limitations in transporting child(ren) to and from day care program? ¨ Yes |
¨ No |
||||
If “yes”, describe: _______________________________________________________________
nyc
ACD 1019 (REVERSE)ACS REV 6/02
NYC Administration for
Children’s Services
3. Reason for Day Care
Explain why day care is needed and how day care will aid the family and/or child(ren). Include service plan for family and/or child(ren). If recertification, update service plan to show progress or current status and explain why day care is still needed. A SERVICE OR TREATMENT PLAN MUST BE INCLUDED WITH THIS REFERRAL. Attach any additional sheets required.
4. Current Family Social Functioning
Give any additional information that might be useful in attempting to make an appropriate day care placement for the child(ren); I . E . , specifics regarding physical or emotional health, family relationships, school problems (for
Referring Person
Name (Print):__________________________________________ |
Tel. No.: _________________ |
Signature: ____________________________________________ |
Date: _____ /______ /_____ |
|
|
Supervisor |
|
|
|
Name (Print):__________________________________________ |
Tel. No.: _________________ |
Signature: __________________________________________ |
Date: _____ /______ /_____ |
|
|