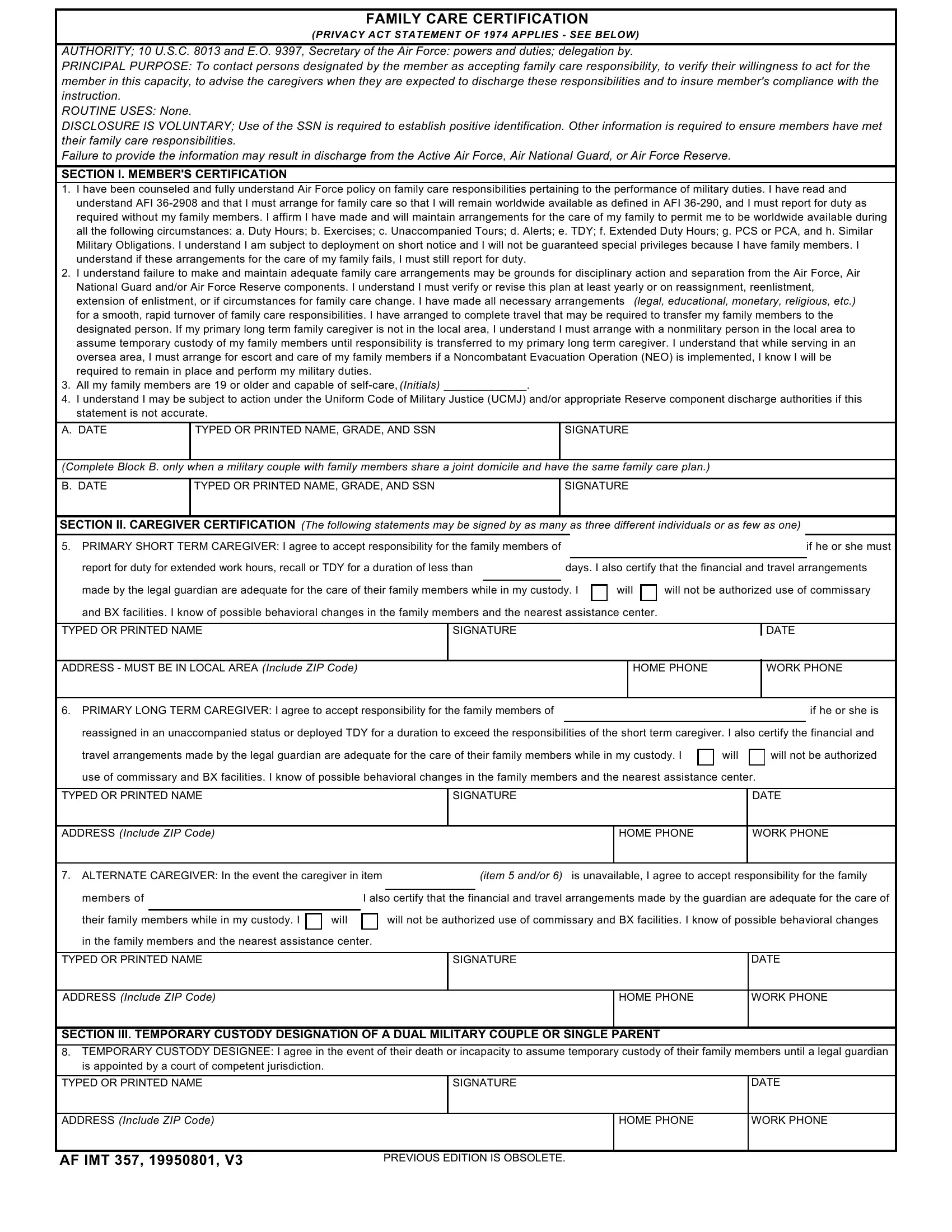
In ensuring the readiness and efficiency of its active duty personnel, the United States Air Force employs the AF IMT 357 form, a document of paramount importance in the orchestration of family care plans. This form, underpinned by the authority of 10 U.S.C. 8013 and Executive Order 9397, mandates the identification of responsible individuals who are willing and able to assume the care of service members' family members during periods of military obligation that may include duty hours, exercises, deployments, and other similar commitments. The principal aim of the AF IMT 357 is to maintain the service member's worldwide availability by ensuring that family care responsibilities do not impede their military duties. Disclosure through this form, while voluntary, is intensely encouraged as failure to establish and maintain adequate family care arrangements can lead to disciplinary action or even separation from military service. Through this detailed documentation process, which requires annual verification or updates in response to family or service status changes, the Air Force seeks to mitigate the potential for family care issues that could detract from mission readiness and effectiveness.
| Question | Answer |
|---|---|
| Form Name | Form Af Imt 357 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | form af, af imt 357, af certification, af 357 |
FAMILY CARE CERTIFICATION
(PRIVACY ACT STATEMENT OF 1974 APPLIES - SEE BELOW)
AUTHORITY; 10 U.S.C. 8013 and E.O. 9397, Secretary of the Air Force: powers and duties; delegation by.
PRINCIPAL PURPOSE: To contact persons designated by the member as accepting family care responsibility, to verify their willingness to act for the member in this capacity, to advise the caregivers when they are expected to discharge these responsibilities and to insure member's compliance with the instruction.
ROUTINE USES: None.
DISCLOSURE IS VOLUNTARY; Use of the SSN is required to establish positive identification. Other information is required to ensure members have met their family care responsibilities.
Failure to provide the information may result in discharge from the Active Air Force, Air National Guard, or Air Force Reserve.
SECTION I. MEMBER'S CERTIFICATION
1.I have been counseled and fully understand Air Force policy on family care responsibilities pertaining to the performance of military duties. I have read and understand AFI
2.I understand failure to make and maintain adequate family care arrangements may be grounds for disciplinary action and separation from the Air Force, Air National Guard and/or Air Force Reserve components. I understand I must verify or revise this plan at least yearly or on reassignment, reenlistment,
extension of enlistment, or if circumstances for family care change. I have made all necessary arrangements (legal, educational, monetary, religious, etc.) for a smooth, rapid turnover of family care responsibilities. I have arranged to complete travel that may be required to transfer my family members to the designated person. If my primary long term family caregiver is not in the local area, I understand I must arrange with a nonmilitary person in the local area to assume temporary custody of my family members until responsibility is transferred to my primary long term caregiver. I understand that while serving in an oversea area, I must arrange for escort and care of my family members if a Noncombatant Evacuation Operation (NEO) is implemented, I know I will be required to remain in place and perform my military duties.
3.All my family members are 19 or older and capable of
4.I understand I may be subject to action under the Uniform Code of Military Justice (UCMJ) and/or appropriate Reserve component discharge authorities if this statement is not accurate.
A. DATE |
TYPED OR PRINTED NAME, GRADE, AND SSN |
SIGNATURE |
|
|
|
(Complete Block B. only when a military couple with family members share a joint domicile and have the same family care plan.)
B. DATE |
TYPED OR PRINTED NAME, GRADE, AND SSN |
SIGNATURE |
|
|
|
SECTION II. CAREGIVER CERTIFICATION (The following statements may be signed by as many as three different individuals or as few as one)
5.PRIMARY SHORT TERM CAREGIVER: I agree to accept responsibility for the family members of if he or she must
report for duty for extended work hours, recall or TDY for a duration of less than |
days. I also certify that the financial and travel arrangements |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
made by the legal guardian are adequate for the care of their family members while in my custody. I |
|
will |
|
|
will not be authorized use of commissary |
|
|||||
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
and BX facilities. I know of possible behavioral changes in the family members and the nearest assistance center. |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
TYPED OR PRINTED NAME |
SIGNATURE |
|
|
|
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS - MUST BE IN LOCAL AREA (Include ZIP Code)
HOME PHONE
WORK PHONE
6. PRIMARY LONG TERM CAREGIVER: I agree to accept responsibility for the family members of if he or she is reassigned in an unaccompanied status or deployed TDY for a duration to exceed the responsibilities of the short term caregiver. I also certify the financial and
travel arrangements made by the legal guardian are adequate for the care of their family members while in my custody. I |
|
will |
|
will not be authorized |
|
|
|
|
|
|
|
use of commissary and BX facilities. I know of possible behavioral changes in the family members and the nearest assistance center. |
|||||
|
|
|
|
|
|
TYPED OR PRINTED NAME |
SIGNATURE |
|
|
DATE |
|
|
|
|
|
|
|
ADDRESS (Include ZIP Code)
HOME PHONE
WORK PHONE
7. ALTERNATE CAREGIVER: In the event the caregiver in item |
|
|
(item 5 and/or 6) is unavailable, I agree to accept responsibility for the family |
|||||||
|
|
|
|
|
|
|
|
|
||
members of |
|
|
I also certify that the financial and travel arrangements made by the guardian are adequate for the care of |
|||||||
|
|
|
|
|
|
|
|
|
|
|
their family members while in my custody. I |
|
will |
|
|
will not be authorized use of commissary and BX facilities. I know of possible behavioral changes |
|||||
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
in the family members and the nearest assistance center. |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
TYPED OR PRINTED NAME |
|
|
|
|
|
SIGNATURE |
DATE |
|||
|
|
|
|
|
|
|
|
|
|
|
ADDRESS (Include ZIP Code)
HOME PHONE
WORK PHONE
SECTION III. TEMPORARY CUSTODY DESIGNATION OF A DUAL MILITARY COUPLE OR SINGLE PARENT
8.TEMPORARY CUSTODY DESIGNEE: I agree in the event of their death or incapacity to assume temporary custody of their family members until a legal guardian is appointed by a court of competent jurisdiction.
TYPED OR PRINTED NAME |
SIGNATURE |
DATE |
|
|
|
|
|
ADDRESS (Include ZIP Code)
HOME PHONE
WORK PHONE
AF IMT 357, 19950801, V3
PREVIOUS EDITION IS OBSOLETE.
FAMILY CARE CERTIFICATION
(PRIVACY ACT STATEMENT OF 1974 APPLIES - SEE BELOW)
AUTHORITY; 10 U.S.C. 8013 and E.O. 9397, Secretary of the Air Force: powers and duties; delegation by.
PRINCIPAL PURPOSE: To contact persons designated by the member as accepting family care responsibility, to verify their willingness to act for the member in this capacity, to advise the caregivers when they are expected to discharge these responsibilities and to insure member's compliance with the instruction.
ROUTINE USES: None.
DISCLOSURE IS VOLUNTARY; Use of the SSN is required to establish positive identification. Other information is required to ensure members have met their family care responsibilities.
Failure to provide the information may result in discharge from the Active Air Force, Air National Guard, or Air Force Reserve.
SECTION I. MEMBER'S CERTIFICATION
1.I have been counseled and fully understand Air Force policy on family care responsibilities pertaining to the performance of military duties. I have read and understand AFI
2.I understand failure to make and maintain adequate family care arrangements may be grounds for disciplinary action and separation from the Air Force, Air National Guard and/or Air Force Reserve components. I understand I must verify or revise this plan at least yearly or on reassignment, reenlistment,
extension of enlistment, or if circumstances for family care change. I have made all necessary arrangements (legal, educational, monetary, religious, etc.) for a smooth, rapid turnover of family care responsibilities. I have arranged to complete travel that may be required to transfer my family members to the designated person. If my primary long term family caregiver is not in the local area, I understand I must arrange with a nonmilitary person in the local area to assume temporary custody of my family members until responsibility is transferred to my primary long term caregiver. I understand that while serving in an oversea area, I must arrange for escort and care of my family members if a Noncombatant Evacuation Operation (NEO) is implemented, I know I will be required to remain in place and perform my military duties.
3.All my family members are 19 or older and capable of
4.I understand I may be subject to action under the Uniform Code of Military Justice (UCMJ) and/or appropriate Reserve component discharge authorities if this statement is not accurate.
A. DATE |
TYPED OR PRINTED NAME, GRADE, AND SSN |
SIGNATURE |
|
|
|
(Complete Block B. only when a military couple with family members share a joint domicile and have the same family care plan.)
B. DATE |
TYPED OR PRINTED NAME, GRADE, AND SSN |
SIGNATURE |
|
|
|
SECTION II. CAREGIVER CERTIFICATION (The following statements may be signed by as many as three different individuals or as few as one)
5.PRIMARY SHORT TERM CAREGIVER: I agree to accept responsibility for the family members of if he or she must
report for duty for extended work hours, recall or TDY for a duration of less than |
days. I also certify that the financial and travel arrangements |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
made by the legal guardian are adequate for the care of their family members while in my custody. I |
|
will |
|
|
will not be authorized use of commissary |
|
|||||
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
and BX facilities. I know of possible behavioral changes in the family members and the nearest assistance center. |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
TYPED OR PRINTED NAME |
SIGNATURE |
|
|
|
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS - MUST BE IN LOCAL AREA (Include ZIP Code)
HOME PHONE
WORK PHONE
6. PRIMARY LONG TERM CAREGIVER: I agree to accept responsibility for the family members of if he or she is reassigned in an unaccompanied status or deployed TDY for a duration to exceed the responsibilities of the short term caregiver. I also certify the financial and
travel arrangements made by the legal guardian are adequate for the care of their family members while in my custody. I |
|
will |
|
will not be authorized |
|
|
|
|
|
|
|
use of commissary and BX facilities. I know of possible behavioral changes in the family members and the nearest assistance center. |
|||||
|
|
|
|
|
|
TYPED OR PRINTED NAME |
SIGNATURE |
|
|
DATE |
|
|
|
|
|
|
|
ADDRESS (Include ZIP Code)
HOME PHONE
WORK PHONE
7. ALTERNATE CAREGIVER: In the event the caregiver in item |
|
|
(item 5 and/or 6) is unavailable, I agree to accept responsibility for the family |
|||||||
|
|
|
|
|
|
|
|
|
||
members of |
|
|
I also certify that the financial and travel arrangements made by the guardian are adequate for the care of |
|||||||
|
|
|
|
|
|
|
|
|
|
|
their family members while in my custody. I |
|
will |
|
|
will not be authorized use of commissary and BX facilities. I know of possible behavioral changes |
|||||
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
in the family members and the nearest assistance center. |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
TYPED OR PRINTED NAME |
|
|
|
|
|
SIGNATURE |
DATE |
|||
|
|
|
|
|
|
|
|
|
|
|
ADDRESS (Include ZIP Code)
HOME PHONE
WORK PHONE
SECTION III. TEMPORARY CUSTODY DESIGNATION OF A DUAL MILITARY COUPLE OR SINGLE PARENT
8.TEMPORARY CUSTODY DESIGNEE: I agree in the event of their death or incapacity to assume temporary custody of their family members until a legal guardian is appointed by a court of competent jurisdiction.
TYPED OR PRINTED NAME |
SIGNATURE |
DATE |
|
|
|
|
|
ADDRESS (Include ZIP Code)
HOME PHONE
WORK PHONE
AF IMT 357, 19950801, V3
PREVIOUS EDITION IS OBSOLETE.
AF IMT 357, BLANK CONTINUATION SHEET.