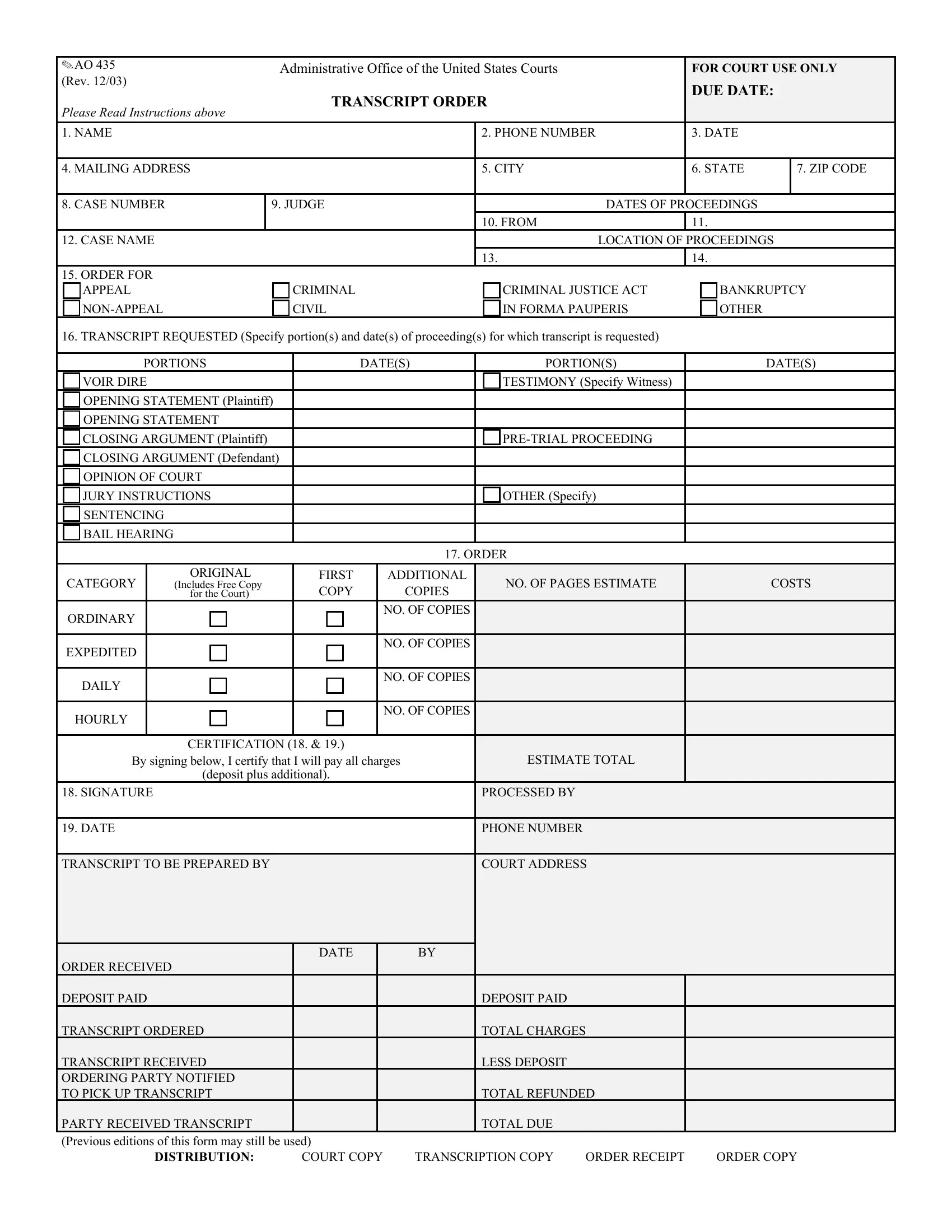
Within the framework of legal proceedings in the United States, the AO 435 form emerges as a critical document, primarily utilized by the Administrative Office of the United States Courts. This form, designated explicitly for court use and detailed in its latest revision as of December 2003, serves as a formal request for the transcription of court proceedings. It encompasses a comprehensive structure that requires the inclusion of various details by the requesting party, such as the name, contact information, and mailing address, alongside the specifics of the case—ranging from the case number to the involved judge's name. Further intricacy is added as the form categorizes requests based on the nature of the case, be it for appeal or non-appeal purposes, and identifies the type of proceedings, including criminal, civil, and others like bankruptcy or those under the Criminal Justice Act or in forma pauperis conditions. What underscores the significance of the AO 435 form is its role in specifying the exact portions of proceedings for which a transcript is necessary, which could include anything from voir dire testimony to sentencing or bail hearings, thereby facilitating a tailored approach to transcript requests. Additionally, the form delineates instructions for estimating the costs associated with the transcription service, encompassing rates for different delivery speeds and the number of copies requested, and it underscores the financial responsibility of the requesting party through a certification process. The completion and processing of this document thereby become a pivotal step in ensuring access to official court records, requisite for various post-proceeding activities, including appeals, compliance, and legal analysis.
| Question | Answer |
|---|---|
| Form Name | Form Ao 435 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ao435 transcript order form ao 435 |
✎ AO 435 |
Administrative Office of the United States Courts |
|
FOR COURT USE ONLY |
||
(Rev. 12/03) |
|
|
|
DUE DATE: |
|
|
|
|
|
|
|
PLEASE READ INSTRUCTIONS ABOVE |
TRANSCRIPT ORDER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. NAME |
|
2. PHONE NUMBER |
|
3. DATE |
|
|
|
|
|
|
|
4. MAILING ADDRESS |
|
5. CITY |
|
6. STATE |
7. ZIP CODE |
|
|
|
|
|
|
8. CASE NUMBER |
9. JUDGE |
|
DATES OF PROCEEDINGS |
|
|
|
|
10. FROM |
|
11. |
|
12. CASE NAME |
|
|
LOCATION OF PROCEEDINGS |
|
|
|
|
13. |
|
14. |
|
15.ORDER FOR APPEAL
CRIMINAL CIVIL
CRIMINAL JUSTICE ACT IN FORMA PAUPERIS
BANKRUPTCY OTHER
16. TRANSCRIPT REQUESTED (Specify portion(s) and date(s) of proceeding(s) for which transcript is requested)
|
|
PORTIONS |
|
DATE(S) |
PORTION(S) |
DATE(S) |
||||
|
|
VOIR DIRE |
|
|
|
|
TESTIMONY (Specify Witness) |
|
|
|
|
|
OPENING STATEMENT (Plaintiff) |
|
|
|
|
|
|
||
|
|
OPENING STATEMENT |
|
|
|
|
|
|
||
|
|
CLOSING ARGUMENT (Plaintiff) |
|
|
|
|
|
|||
|
|
CLOSING ARGUMENT (Defendant) |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|||
|
|
OPINION OF COURT |
|
|
|
|
|
|
||
|
|
JURY INSTRUCTIONS |
|
|
|
OTHER (Specify) |
|
|
||
|
|
SENTENCING |
|
|
|
|
|
|
|
|
|
|
BAIL HEARING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17. ORDER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CATEGORY |
|
ORIGINAL |
FIRST |
|
ADDITIONAL |
NO. OF PAGES ESTIMATE |
COSTS |
|
|
|
|
(Includes Free Copy |
COPY |
|
COPIES |
|
||||
|
|
|
|
for the Court) |
|
|
|
|
||
|
ORDINARY |
|
|
|
|
NO. OF COPIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
EXPEDITED |
|
|
|
|
NO. OF COPIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
DAILY |
|
|
|
|
NO. OF COPIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOURLY |
|
|
|
|
NO. OF COPIES |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CERTIFICATION (18. & 19.) |
|
|
|
|
|
|
|
|
By signing below, I certify that I will pay all charges |
ESTIMATE TOTAL |
|
|
|||||
|
|
|||||||||
|
|
|
|
(deposit plus additional). |
|
|
|
|
|
|
18. SIGNATURE |
|
|
|
|
PROCESSED BY |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
19. DATE |
|
|
|
|
PHONE NUMBER |
|
|
|||
|
|
|
|
|
|
|
|
|
||
TRANSCRIPT TO BE PREPARED BY |
|
|
|
COURT ADDRESS |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
DATE |
BY |
|
|
|
|
ORDER RECEIVED |
|
|
|
|
|
|
DEPOSIT PAID |
|
|
DEPOSIT PAID |
|
|
|
TRANSCRIPT ORDERED |
|
|
TOTAL CHARGES |
|
|
|
TRANSCRIPT RECEIVED |
|
|
LESS DEPOSIT |
|
|
|
ORDERING PARTY NOTIFIED |
|
|
|
|
|
|
TO PICK UP TRANSCRIPT |
|
|
TOTAL REFUNDED |
|
|
|
PARTY RECEIVED TRANSCRIPT |
|
|
TOTAL DUE |
|
|
|
|
|
|
|
|
||
(Previous editions of this form may still be used) |
|
|
|
|
|
|
DISTRIBUTION: |
COURT COPY |
TRANSCRIPTION COPY |
ORDER RECEIPT |
ORDER COPY |
|
|