In the state of Michigan, motor vehicle repair facilities operate under strict regulatory guidelines designed to ensure integrity, compliance, and consumer protection within this critical sector. Central to maintaining these standards is the AR-0175 form, a bureaucratic instrument issued by the Michigan Department of State. This document is earmarked for instances when a repair facility undergoes changes in its cadre of officers, directors, or significant stockholders—individuals owning 10% or more of the company's stock. The form requires detailed personal and professional information about incoming personnel to ensure that those at the helm of these establishments meet the requisite legal and ethical standards. Notably, it acts as a safeguard, preventing entities that have undergone substantial structural changes from bypassing the rigorous scrutiny applied to new market entrants. Moreover, the AR-0175 form includes provisions for disclosing previous engagement in motor vehicle repair enterprises and any criminal convictions, thereby offering a holistic view of the applicant's history. This level of transparency is crucial for maintaining public trust and ensuring that the Michigan automotive repair industry operates to the highest standards. Compliance with this form and understanding its implications is essential for anyone involved in the administration of a motor vehicle repair facility in Michigan, signifying a commitment to uprightness and accountability within the industry.
| Question | Answer |
|---|---|
| Form Name | Form Ar 0175 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ar0175_24392_7 michigan gov motor vehicle repair facility form |

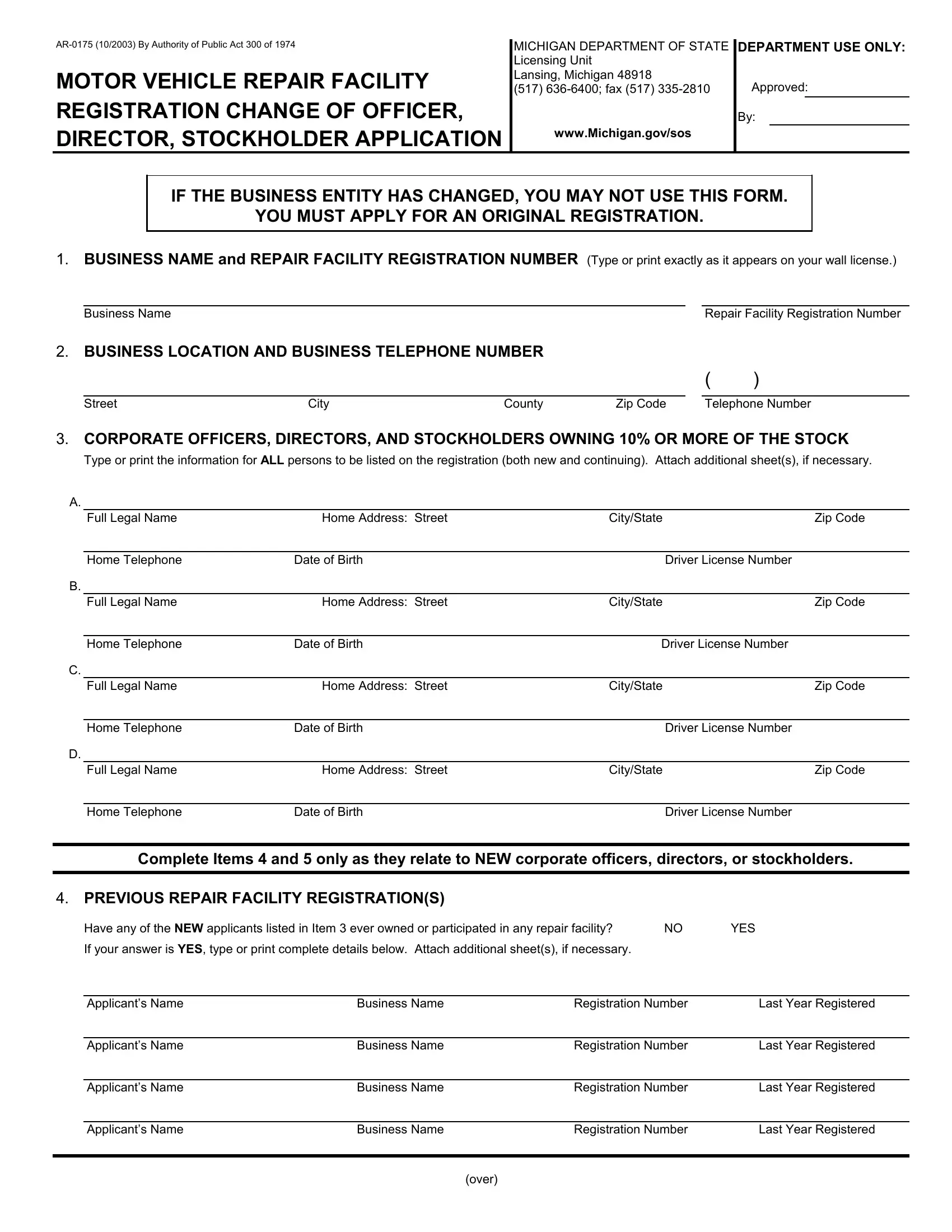
MOTOR VEHICLE REPAIR FACILITY REGISTRATION CHANGE OF OFFICER, DIRECTOR, STOCKHOLDER APPLICATION
MICHIGAN DEPARTMENT OF STATE
Licensing Unit
Lansing, Michigan 48918
(517)
www.Michigan.gov/sos
DEPARTMENT USE ONLY:
Approved:
By:
IF THE BUSINESS ENTITY HAS CHANGED, YOU MAY NOT USE THIS FORM.
YOU MUST APPLY FOR AN ORIGINAL REGISTRATION.
1.BUSINESS NAME and REPAIR FACILITY REGISTRATION NUMBER (Type or print exactly as it appears on your wall license.)
Business Name |
Repair Facility Registration Number |
2.BUSINESS LOCATION AND BUSINESS TELEPHONE NUMBER
( )
Street |
City |
County |
Zip Code |
Telephone Number |
3.CORPORATE OFFICERS, DIRECTORS, AND STOCKHOLDERS OWNING 10% OR MORE OF THE STOCK
Type or print the information for ALL persons to be listed on the registration (both new and continuing). Attach additional sheet(s), if necessary.
A.
|
Full Legal Name |
Home Address: Street |
City/State |
Zip Code |
|
|
|
|
|
|
Home Telephone |
Date of Birth |
Driver License Number |
|
B. |
|
|
|
|
|
Full Legal Name |
Home Address: Street |
City/State |
Zip Code |
|
|
|
|
|
|
Home Telephone |
Date of Birth |
Driver License Number |
|
C. |
|
|
|
|
|
Full Legal Name |
Home Address: Street |
City/State |
Zip Code |
|
|
|
|
|
|
Home Telephone |
Date of Birth |
Driver License Number |
|
D. |
|
|
|
|
|
Full Legal Name |
Home Address: Street |
City/State |
Zip Code |
|
|
|
|
|
|
Home Telephone |
Date of Birth |
Driver License Number |
|
Complete Items 4 and 5 only as they relate to NEW corporate officers, directors, or stockholders.
4.PREVIOUS REPAIR FACILITY REGISTRATION(S)
Have any of the NEW applicants listed in Item 3 ever owned or participated in any repair facility? ¸ NO |
¸ YES |
||
If your answer is YES, type or print complete details below. Attach additional sheet(s), if necessary. |
|
||
|
|
|
|
Applicant’s Name |
Business Name |
Registration Number |
Last Year Registered |
|
|
|
|
Applicant’s Name |
Business Name |
Registration Number |
Last Year Registered |
|
|
|
|
Applicant’s Name |
Business Name |
Registration Number |
Last Year Registered |
|
|
|
|
Applicant’s Name |
Business Name |
Registration Number |
Last Year Registered |
(over)
5.ARRESTS OR CONVICTIONS
Have any of the NEW applicants listed in Item 3 been arrested or convicted of a crime other than a traffic violation in Michigan or any other state within the past ten (10) years? ¸ NO ¸ YES
If your answer is YES, type or print the name(s) of the applicant(s) involved and complete details of all arrests or convictions that took place in the past ten (10) years. Attach additional sheet(s), if necessary.
Name(s) of Person(s) Arrested or Convicted, and Details
Enter Details Here:
Date(s) of Arrest(s) or Conviction(s) Enter Dates Here:
Court(s) of Record Enter Court(s) of Record here:
City and State
Enter City and State Here:
6.READ CAREFULLY BEFORE SIGNING. ALL PERSONS LISTED IN ITEM 3 MUST SIGN.
I certify that the statements contained in this application are true and I, as an officer, director, or stockholder of the corporation, have authority to sign this application and to make the statements contained herein. I understand that any misleading, incomplete, or false statement shall be grounds for denial of this application or the suspension or revocation of my registration.
I stipulate and agree that any legal process affecting this business served on the Secretary of State or his/her deputies shall have the same effect as if personally served on me and all other owners of this business, if any. I further agree that this appointment shall remain in force as long as any liability of this business remains outstanding within the State of Michigan.
|
Signature |
Title |
Date |
|
|
|
|
|
Signature |
Title |
Date |
|
|
|
|
|
Signature |
Title |
Date |
|
|
|
|
|
Signature |
Title |
Date |
|
|
|
|
|
Signature |
Title |
Date |
|
|
|
|
|
Signature |
Title |
Date |
|
|
|
|