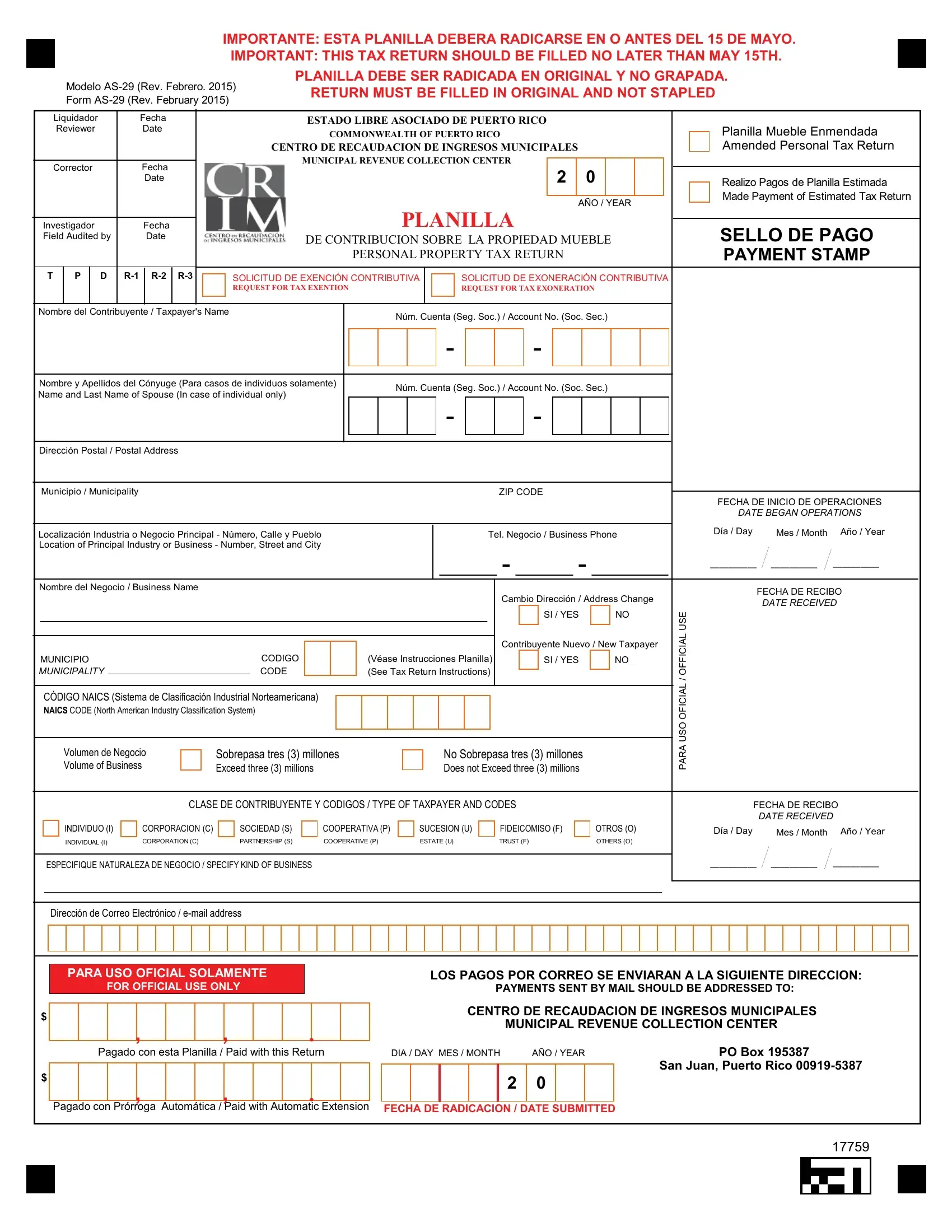
Navigating the intricacies of tax documentation is crucial for maintaining compliance and managing financial responsibilities effectively. The AS-29 form, revised in February 2015, serves as a fundamental document for entities in Puerto Rico to detail their personal property taxes. This form, essential for both individuals and businesses, must be submitted by the strict deadline of May 15th every year to the Municipal Revenue Collection Center. The primary purpose of the AS-29 is to facilitate the declaration and calculation of taxes on movable properties, acknowledging both payments made and exemptions applicable. It includes sections for amended returns, estimated tax payments, tax exoneration requests, and detailed financial breakdowns. Moreover, it caters to diverse taxpayer types, ranging from individuals and corporations to partnerships and trusts, each with its classifications and codes. Compliance with the stipulations, such as original submission without staples and adherence to official municipality codes, is emphasized. AS-29 not only underscores the taxpayer's responsibility towards municipal contributions but also offers provisions for exemptions and discounts under specific conditions, making it an indispensable tool for fiscal management within the Commonwealth of Puerto Rico.
| Question | Answer |
|---|---|
| Form Name | Form As 29 |
| Form Length | 25 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 6 min 15 sec |
| Other names | puerto rico form as 29 pdf, 29 form as, as form 29, crim as 29 form |
IMPORTANTE: ESTA PLANILLA DEBERA RADICARSE EN O ANTES DEL 15 DE MAYO.
IMPORTANT: THIS TAX RETURN SHOULD BE FILLED NO LATER THAN MAY 15TH.
PLANILLA DEBE SER RADICADA EN ORIGINAL Y NO GRAPADA.
Modelo
Form
|
Liquidador |
|
Fecha |
|
|
|
|
ESTADO LIBRE ASOCIADO DE PUERTO RICO |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
|
Reviewer |
|
Date |
|
|
|
|
COMMONWEALTH OF PUERTO RICO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Planilla Mueble Enmendada |
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CENTRO DE RECAUDACION DE INGRESOS MUNICIPALES |
|
|
|
|
|
|
|
|
Amended Personal Tax Return |
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
MUNICIPAL REVENUE COLLECTION CENTER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
Corrector |
|
Fecha |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
0 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Realizo Pagos de Planilla Estimada |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Made Payment of Estimated Tax Return |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLANILLA |
|
|
|
|
|
AÑO / YEAR |
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
Investigador |
|
Fecha |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SELLO DE PAGO |
|||||||||||||||||||||||||||
|
Field Audited by |
|
|
Date |
|
|
|
|
DE CONTRIBUCION SOBRE LA PROPIEDAD MUEBLE |
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PERSONAL PROPERTY TAX RETURN |
|
|
|
|
|
|
|
|
PAYMENT STAMP |
||||||||||||||||||||||||||||||||
|
T |
P |
D |
|
|
|
SOLICITUD DE EXENCIÓN CONTRIBUTIVA |
|
|
|
|
SOLICITUD DE EXONERACIÓN CONTRIBUTIVA |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
REQUEST FOR TAX EXENTION |
|
|
|
|
|
|
|
|
|
|
|
|
REQUEST FOR TAX EXONERATION |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nombre del Contribuyente / Taxpayer's Name |
|
|
|
|
|
Núm. Cuenta (Seg. Soc.) / Account No. (Soc. Sec.) |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nombre y Apellidos del Cónyuge (Para casos de individuos solamente) |
|
|
|
|
|
Núm. Cuenta (Seg. Soc.) / Account No. (Soc. Sec.) |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
Name and Last Name of Spouse (In case of individual only) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dirección Postal / Postal Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Municipio / Municipality |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FECHA DE INICIO DE OPERACIONES |
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE BEGAN OPERATIONS |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Día / Day |
Mes / Month |
Año / Year |
|||||||||
Localización Industria o Negocio Principal - Número, Calle y Pueblo |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tel. Negocio / Business Phone |
|
|
|
|||||||||||||||||||||||||||||||||||||||||
Location of Principal Industry or Business - Number, Street and City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
_____ |
_____ |
_____ |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nombre del Negocio / Business Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cambio Dirección / Address Change |
|
|
|
|
FECHA DE RECIBO |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE RECEIVED |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SI / YES |
|
NO |
USE |
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OFFICIAL |
|
|
|
||||||||||||
MUNICIPALITY |
|
|
|
|
|
|
|
CODE |
|
|
(See Tax Return Instructions) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
MUNICIPIO |
|
|
|
|
|
|
|
CODIGO |
|
|
|
|
|
|
(Véase Instrucciones Planilla) |
|
|
Contribuyente Nuevo / New Taxpayer |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SI / YES |
|
NO |
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OFICIALUSO |
|
|
|
|||
|
CÓDIGO NAICS (Sistema de Clasificación Industrial Norteamericana) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
NAICS CODE (North American Industry Classification System) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PARA |
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Volumen de Negocio |
|
Sobrepasa tres (3) millones |
|
|
|
|
|
|
|
|
|
|
|
No Sobrepasa tres (3) millones |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
Volume of Business |
|
Exceed three (3) millions |
|
|
|
|
|
|
|
|
|
|
|
Does not Exceed three (3) millions |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
CLASE DE CONTRIBUYENTE Y CODIGOS / TYPE OF TAXPAYER AND CODES |
|
|
FECHA DE RECIBO |
|
||||
|
|
|
|
|
|
|
|
DATE RECEIVED |
|
INDIVIDUO (I) |
CORPORACION (C) |
SOCIEDAD (S) |
COOPERATIVA (P) |
SUCESION (U) |
FIDEICOMISO (F) |
OTROS (O) |
Día / Day |
Mes / Month |
Año / Year |
INDIVIDUAL (I) |
CORPORATION (C) |
PARTNERSHIP (S) |
COOPERATIVE (P) |
ESTATE (U) |
TRUST (F) |
OTHERS (O) |
|
|
|
|
|
|
_____ _____ _____ |
||
ESPECIFIQUE NATURALEZA DE NEGOCIO / SPECIFY KIND OF BUSINESS |
|
|
|
|
|||
Dirección de Correo Electrónico /
$
$
PARA USO OFICIAL SOLAMENTE |
|
|
|
|
|
|
|
LOS PAGOS POR CORREO SE ENVIARAN A LA SIGUIENTE DIRECCION: |
|||||||||||||||
|
FOR OFFICIAL USE ONLY |
|
|
|
|
|
|
|
|
|
PAYMENTS SENT BY MAIL SHOULD BE ADDRESSED TO: |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CENTRO DE RECAUDACION DE INGRESOS MUNICIPALES |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
, |
|
|
, |
|
. |
|
|
|
|
|
|
|
|
MUNICIPAL REVENUE COLLECTION CENTER |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PO Box 195387 |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Pagado con esta Planilla / Paid with this Return |
|
|
DIA / DAY MES / MONTH |
AÑO / YEAR |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
San Juan, Puerto Rico |
|
|
|
, |
|
|
, |
|
. |
|
|
|
|
|
|
|
|
2 |
0 |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Pagado con Prórroga Automática / Paid with Automatic Extension |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
FECHA DE RADICACION |
/ DATE SUBMITTED |
|
|||||||||||||||||||
17759