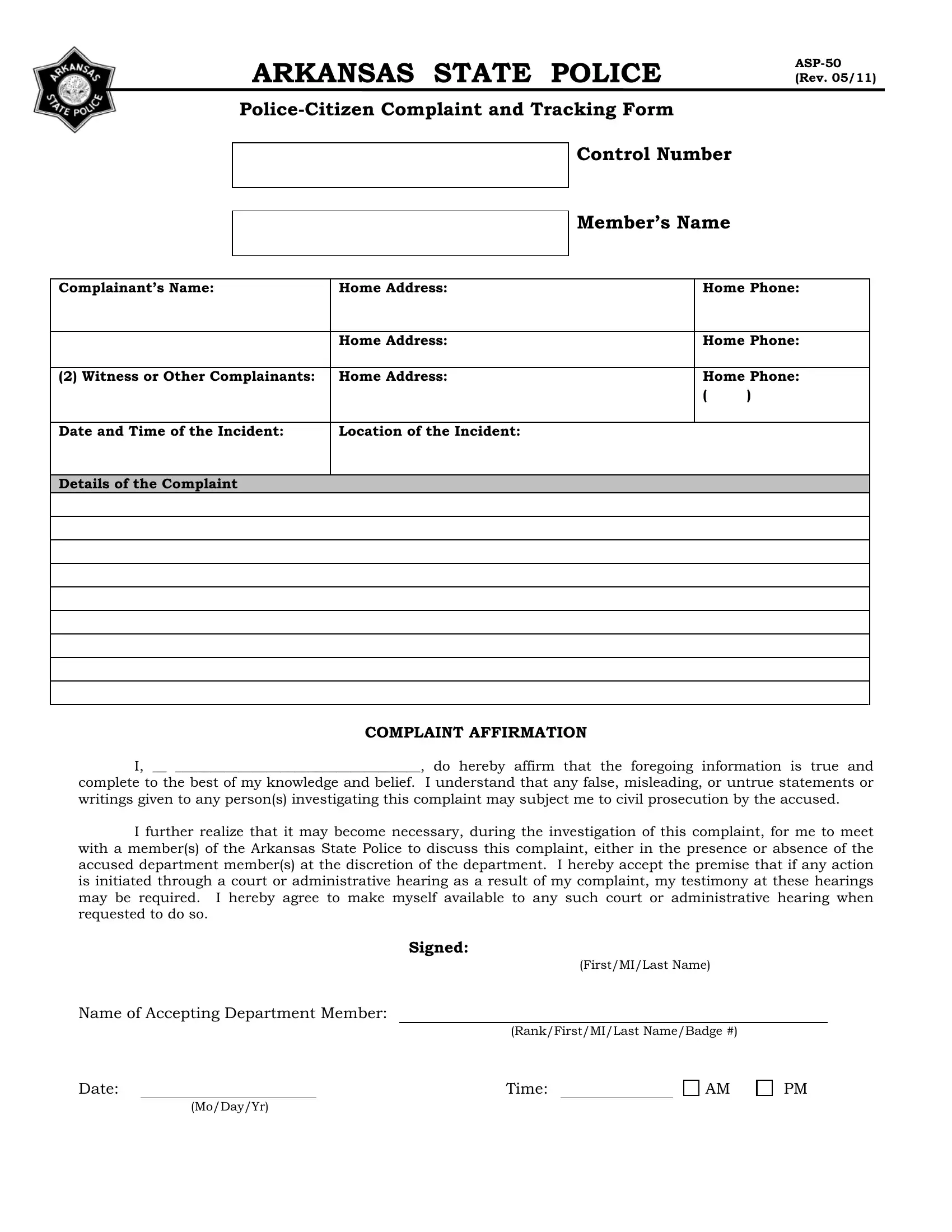
The Asp 50 form plays a pivotal role in the process of filing and tracking complaints against members of the Arkansas State Police, fostering transparency and accountability within the organization. This document, officially known as the Police-Citizen Complaint and Tracking Form, offers a structured way for individuals to report their grievances related to the conduct of police personnel. It captures essential details such as the complainant's name, contact information, the involved officer's name, date and time of the incident, and a thorough description of the complaint. Moreover, it emphasizes the importance of truthfulness by requiring a complaint affirmation, warning of potential civil prosecution for false claims. The process outlined in the form considers various phases of the complaint's lifecycle, from its initiation, through investigation by the department, to the final disposition which could range from no action to termination. It also delineates the roles of different authorities within the department responsible for the oversight of the complaint, including the Office of Professional Standards Officer, Deputy Director, and the Command Staff Review Board. This form underscores the department's commitment to handling citizen complaints with seriousness and diligence, ensuring that any necessary follow-up, including possible court or administrative hearings, is conducted fairly and promptly.
| Question | Answer |
|---|---|
| Form Name | Form Asp 50 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | foregoing, filing a complaint online of arkansas state troopers, inter, Administratively |
ARKANSAS STATE POLICE
Member’s Name
Complainant’s Name: |
Home Address: |
Home Phone: |
|
|
|
|
|
|
Home Address: |
Home Phone: |
|
|
|
|
|
(2) Witness or Other Complainants: |
Home Address: |
Home Phone: |
|
|
|
( |
) |
|
|
|
|
Date and Time of the Incident: |
Location of the Incident: |
|
|
|
|
|
|
Details of the Complaint |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPLAINT AFFIRMATION
I, __ ___________________________________, do hereby affirm that the foregoing information is true and
complete to the best of my knowledge and belief. I understand that any false, misleading, or untrue statements or writings given to any person(s) investigating this complaint may subject me to civil prosecution by the accused.
I further realize that it may become necessary, during the investigation of this complaint, for me to meet with a member(s) of the Arkansas State Police to discuss this complaint, either in the presence or absence of the accused department member(s) at the discretion of the department. I hereby accept the premise that if any action is initiated through a court or administrative hearing as a result of my complaint, my testimony at these hearings may be required. I hereby agree to make myself available to any such court or administrative hearing when requested to do so.
Signed:
(First/MI/Last Name)
Name of Accepting Department Member:
(Rank/First/MI/Last Name/Badge #)
Date: |
|
Time: |
|
AM |
(Mo/Day/Yr)
PM
Date Received:
Assigned To:
Control Number:
Type of Complaint:
A -
Date Investigation Initiated:
Date Investigation Terminated:
Date Forwarded to Deputy Director:
Signature of Office of Professional Standards Officer:
Date of Review:
Signature of Deputy Director:
Command Staff Review Board Chairman/Commander’s Determination: (Check One)
Founded
Unfounded
Inconclusive
Administratively Closed
Comments:
Signature of Command Staff Review Board
Chairman/Commander:
Date Forwarded to Deputy Director:
Date of Review:
Signature of Deputy Director:
FINAL DISPOSITION (CHECK ONE)
No Action Taken
Oral Reprimand/Counseling Letter of Reprimand
Transfer
Suspension
Reduction in Grade/Rank
Termination Other
Comments/Final Recommendations
Director’s Signature: ________________________________________ |
Date: _______________________ |
(Rank/First/MI/Last Name/Badge #) |
(Mo/Day/Yr) |