
Handling PDF documents online is actually a breeze using our PDF editor. You can fill out false here in a matter of minutes. To maintain our tool on the leading edge of practicality, we aim to adopt user-driven features and enhancements regularly. We are always glad to receive feedback - join us in remolding PDF editing. To begin your journey, take these simple steps:
Step 1: Firstly, open the tool by pressing the "Get Form Button" above on this site.
Step 2: Using this advanced PDF tool, you can actually do more than merely fill in blanks. Edit away and make your forms look high-quality with customized textual content added in, or optimize the file's original content to perfection - all comes along with an ability to add any photos and sign the document off.
This form will involve specific information; to ensure consistency, be sure to take heed of the following recommendations:
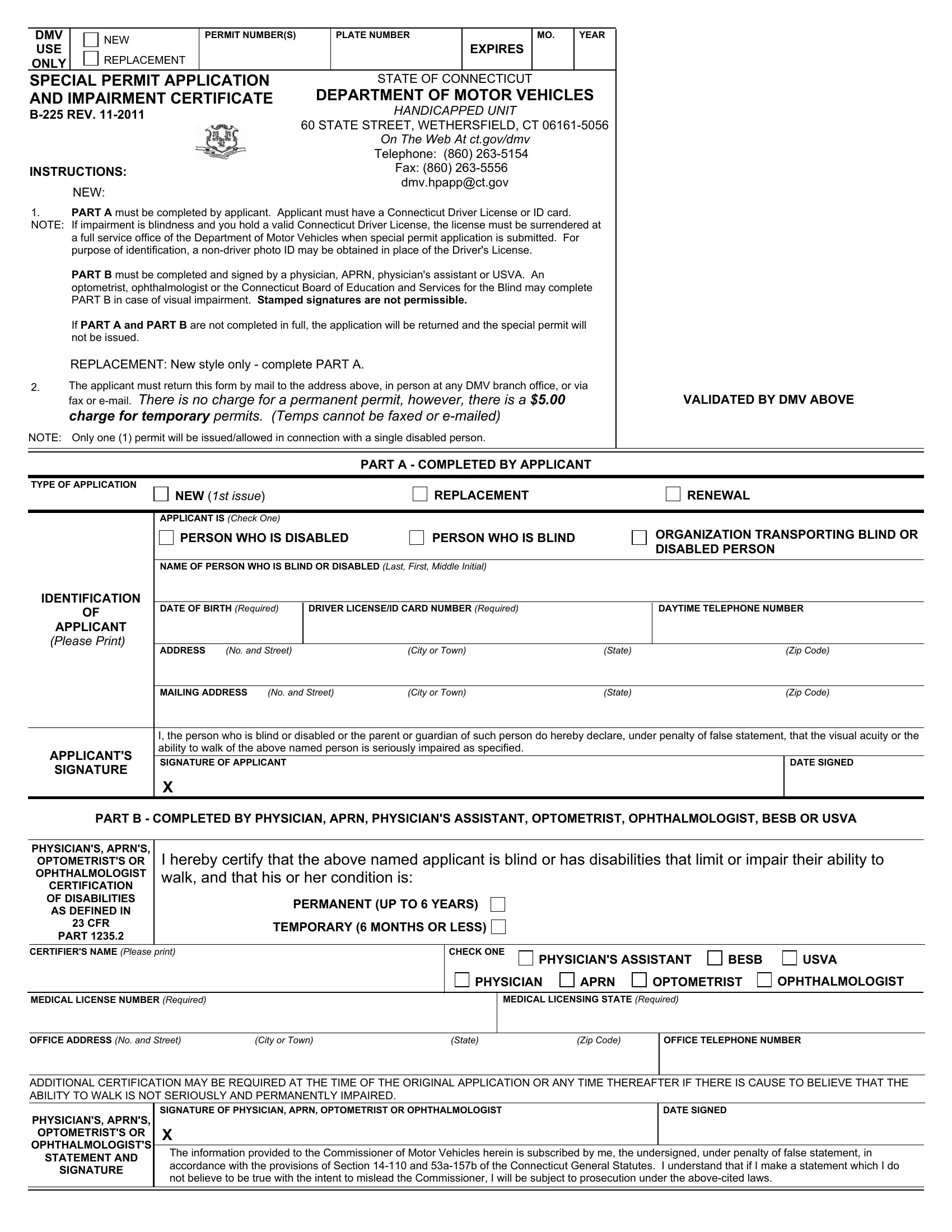
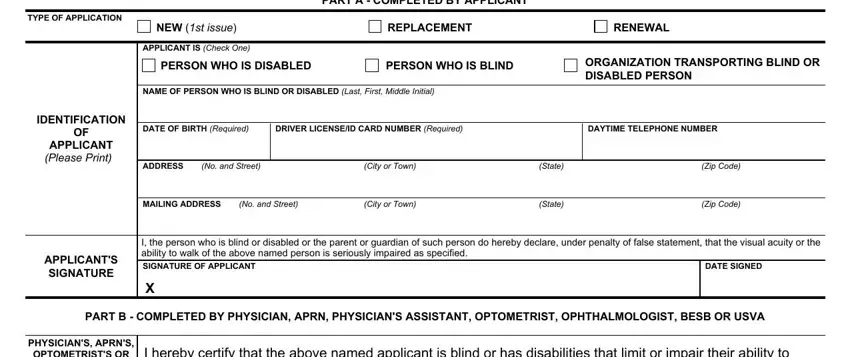
1. It is crucial to complete the false correctly, so be attentive when filling out the segments containing all these blanks:
2. After finishing this step, go to the subsequent stage and enter the essential details in all these fields - OPTOMETRISTS OR OPHTHALMOLOGIST, CERTIFICATION OF DISABILITIES AS, CFR, PART, I hereby certify that the above, PERMANENT UP TO YEARS, TEMPORARY MONTHS OR LESS, CERTIFIERS NAME Please print, CHECK ONE, PHYSICIANS ASSISTANT, BESB, USVA, MEDICAL LICENSE NUMBER Required, MEDICAL LICENSING STATE Required, and PHYSICIAN.
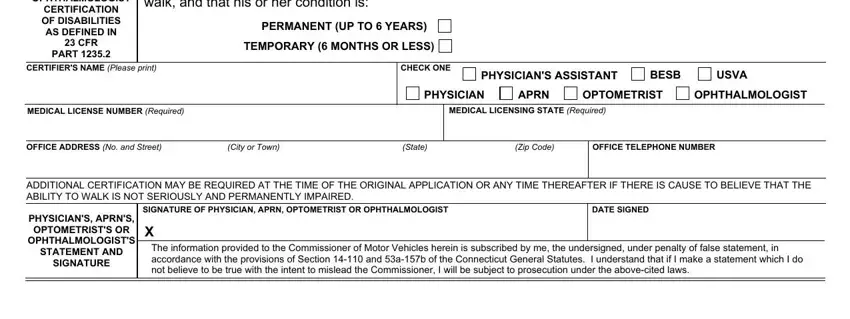
Those who use this PDF generally make mistakes when filling in TEMPORARY MONTHS OR LESS in this section. Ensure that you review everything you enter here.
Step 3: Right after you've reviewed the information in the blanks, simply click "Done" to complete your form. Try a 7-day free trial option with us and gain immediate access to false - download, email, or change from your personal account. We do not sell or share the information you type in whenever completing forms at our website.