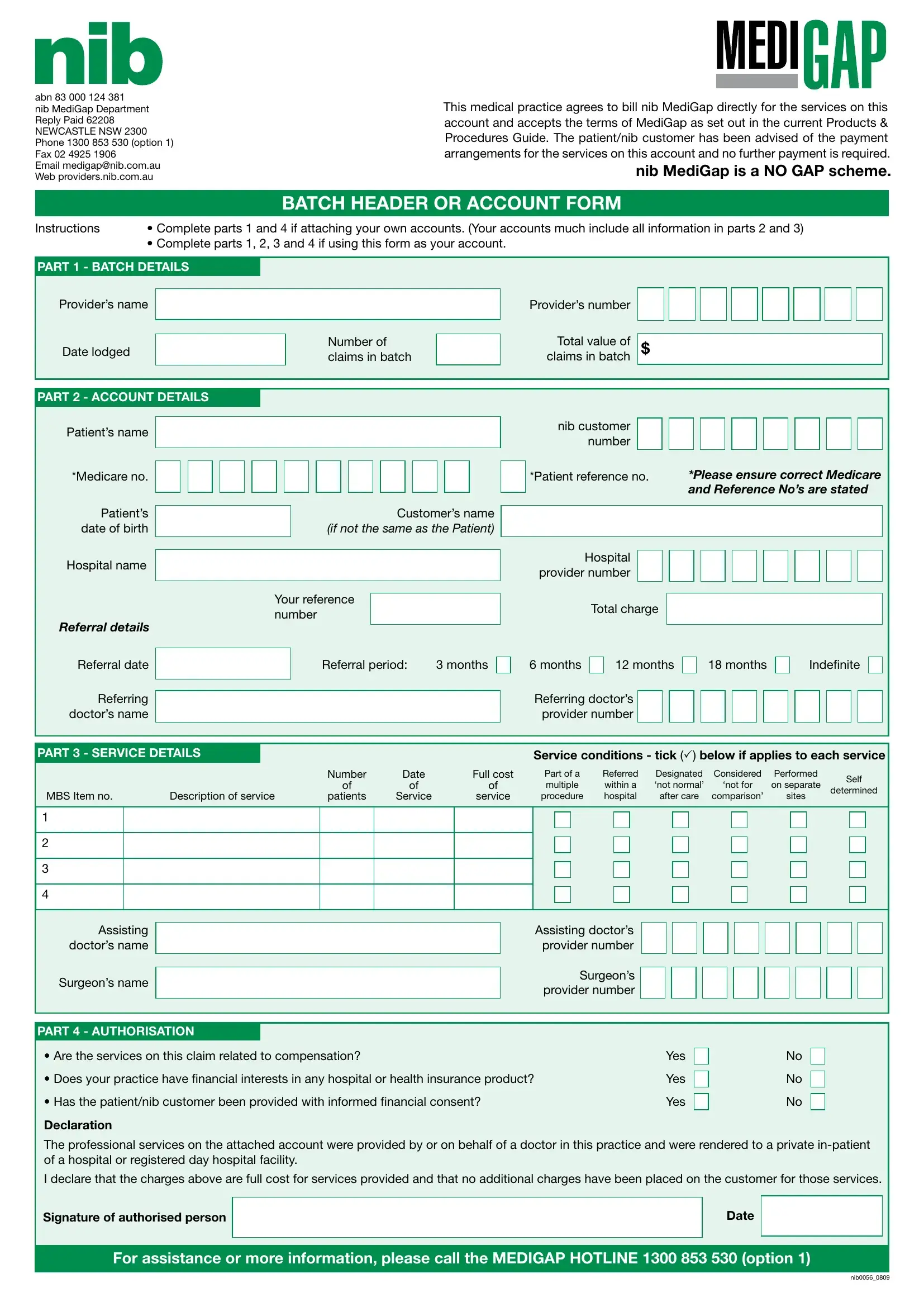
In the realm of healthcare billing and patient care transactions, the Batch Header form embodies a critical document for medical practices aligning with nib MediGap's direct billing protocols. Embedded within this comprehensive form, the essential details span from the medical practice's agreement to bill nib MediGap directly for services rendered to the acclamation of the MediGap scheme as a "NO GAP" initiative, meaning patients are not required to make additional payments for covered services. The form's structure is meticulously divided into several parts, each soliciting specific information ranging from provider and patient details to the intricate service conditions, ensuring a seamless and transparent billing process. Part 1 focuses on batch details such as the provider’s name and total value of claims, while Parts 2 and 3 delve deeper into account and service details, encompassing patient demographics, referral information, and service-specific data. Authorization queries encapsulated in Part 4 render a final check on claims related to compensation cases, financial interests, and informed financial consent from patients. The inclusion of a declaration section further imposes an ethical duty on providers to ensure the truthfulness of their claims. With provisions for both manual and electronic submissions, this form not only streamlines the billing process but equally underlines the commitment between healthcare providers and nib MediGap towards facilitating patient-centric care without the hassle of financial burdens.
| Question | Answer |
|---|---|
| Form Name | Form Batch Header |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | nib provider your, medibank batch header, nib batch header, medibank private batch header |
abn 83 000 124 381
nib MediGap Department Reply Paid 62208 NEWCASTLE NSW 2300 Phone 1300 853 530 (option 1) Fax 02 4925 1906
Email medigap@nib.com.au Web providers.nib.com.au
This medical practice agrees to bill nib MediGap directly for the services on this account and accepts the terms of MediGap as set out in the current Products & Procedures Guide. The patient/nib customer has been advised of the payment arrangements for the services on this account and no further payment is required.
nib MediGap is a NO GAP scheme.
BATCH HEADER OR ACCOUNT FORM
Instructions |
• Complete parts 1 and 4 if attaching your own accounts. (Your accounts much include all information in parts 2 and 3) |
||||||||||||||
|
• Complete parts 1, 2, 3 and 4 if using this form as your account. |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PART 1 - BATCH DETAILS |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Provider’s name |
|
|
|
|
Provider’s number |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Total value of |
|
|
|
|
|
|
|
|
|
|
|
|
Number of |
|
|
|
|
|
|
|
|
|
|
|
Date lodged |
|
|
|
|
|
$ |
|
|
|
|
|
|
|
||
|
|
|
|
claims in batch |
|
|
claims in batch |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PART 2 - ACCOUNT DETAILS
Patient’s name
*Medicare no.
Patient’s date of birth
Hospital name
REFERRAL DETAILS
Referral date
Referring doctor’s name
Customer’s name
(IF NOT THE SAME AS THE PATIENT)
Your reference number
|
Referral period: |
3 months |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
nib customer number
*Patient reference no. |
*PLEASE ENSURE CORRECT MEDICARE |
|
AND REFERENCE NO’S ARE STATED |
Hospital provider number
Total charge
6 months |
|
12 months |
|
18 months |
|
Indeinite |
Referring doctor’s provider number
PART 3 - SERVICE DETAILS |
|
|
|
|
Service conditions - tick () below if applies to each service |
|||||||
|
|
|
Number |
Date |
Full cost |
Part of a |
Referred |
Designated |
Considered |
Performed |
Self |
|
|
|
|
of |
of |
of |
multiple |
within a |
‘not normal’ |
‘not for |
on separate |
||
|
|
|
determined |
|||||||||
MBS Item no. |
Description of service |
patients |
Service |
service |
procedure |
hospital |
after care |
comparison’ |
sites |
|||
|
||||||||||||
1
2
3
4
Assisting doctor’s name
Surgeon’s name
Assisting doctor’s provider number
Surgeon’s provider number
PART 4 - AUTHORISATION |
|
|
|
|
• Are the services on this claim related to compensation? |
Yes |
|
No |
|
|
||||
• Does your practice have inancial interests in any hospital or health insurance product? |
Yes |
|
No |
|
|
||||
• Has the patient/nib customer been provided with informed inancial consent? |
Yes |
|
No |
|
|
||||
Declaration
The professional services on the attached account were provided by or on behalf of a doctor in this practice and were rendered to a private
I declare that the charges above are full cost for services provided and that no additional charges have been placed on the customer for those services.
Signature of authorised person |
|
Date |
|
|
|
For assistance or more information, please call the MEDIGAP HOTLINE 1300 853 530 (option 1)
nib0056_0809