
aged application printable can be filled out effortlessly. Simply try FormsPal PDF editor to get the job done fast. To keep our editor on the forefront of convenience, we work to implement user-driven capabilities and improvements regularly. We're always looking for suggestions - play a vital part in remolding PDF editing. Starting is simple! All that you should do is adhere to these easy steps directly below:
Step 1: Press the "Get Form" button above. It'll open up our tool so you can begin filling in your form.
Step 2: Once you open the online editor, you will see the form all set to be completed. In addition to filling in different blanks, you can also perform other sorts of things with the Document, including putting on custom textual content, editing the original textual content, adding illustrations or photos, signing the PDF, and much more.
It is actually an easy task to fill out the document adhering to this detailed tutorial! Here is what you want to do:
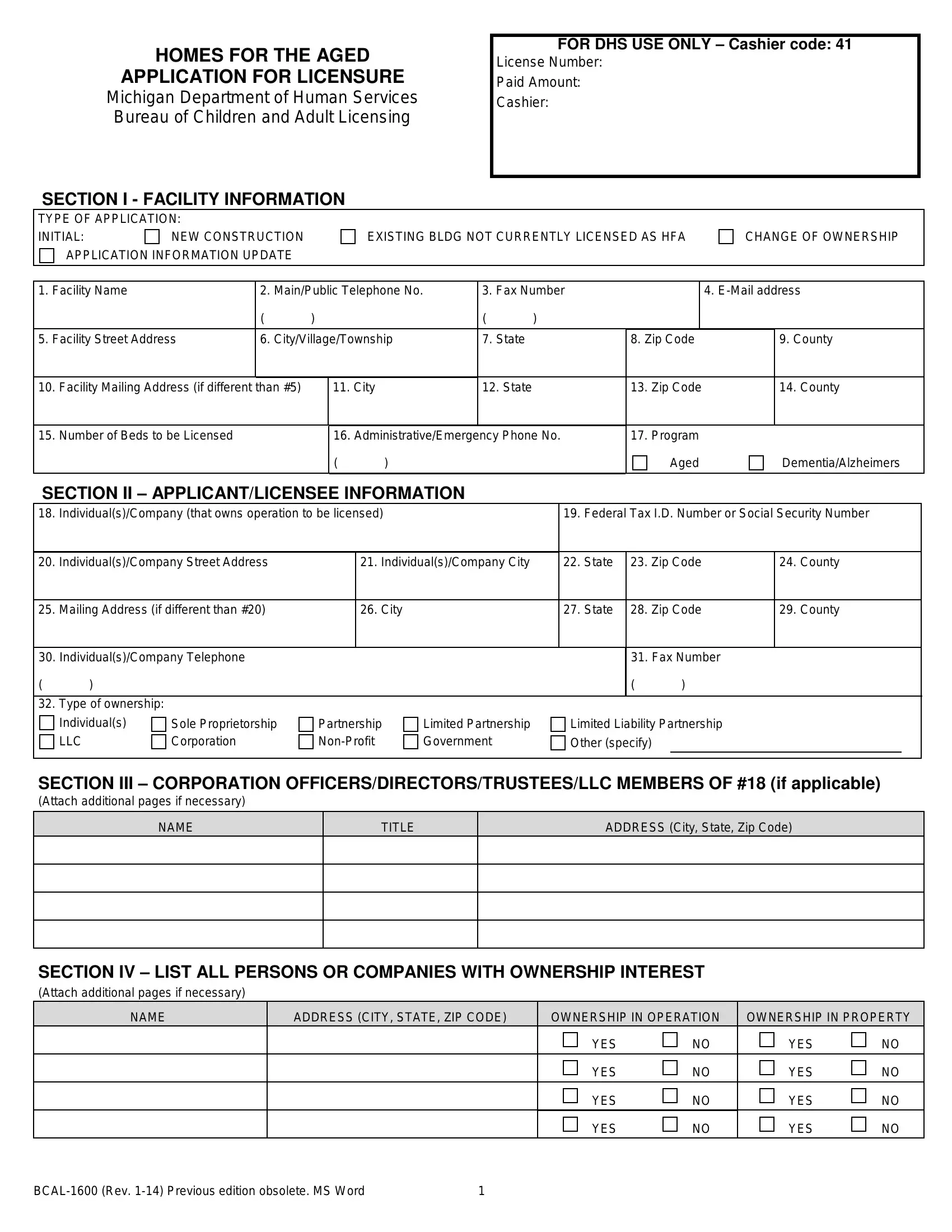
1. To get started, when filling in the aged application printable, start in the section that includes the next fields:
2. Your next part is to fill out these blanks: Number of Beds to be Licensed, AdministrativeEmergency Phone No, Program, Aged, DementiaAlzheimers, SECTION II APPLICANTLICENSEE, IndividualsCompany Street Address, Mailing Address if different than, IndividualsCompany Telephone, Type of ownership, IndividualsCompany City, City, Federal Tax ID Number or Social, State, and Zip Code.
In terms of Mailing Address if different than and Aged, be sure you do everything correctly in this section. These two are surely the most important fields in the PDF.
3. Completing NAME, ADDRESS CITY STATE ZIP CODE, OWNERSHIP IN OPERATION NO NO NO NO, YES YES YES YES, OWNERSHIP IN PROPERTY, YES YES YES YES, NO NO NO NO, and BCAL Rev Previous edition is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. The next section requires your details in the subsequent areas: NAME, ADDRESS City State Zip Code, SECTION VI AUTHORIZED, An authorized representative shall, Authorized Representative, Email Address, Email Address, Social Security, Phone, Alternative Phone Number, Fax Number, Alternative Phone Number, Fax Number, SECTION VII ADMINISTRATOR Use, and Social Security. Just be sure you fill in all of the requested info to move further.
5. To finish your form, this particular section includes several additional fields. Completing Individual Applicant or Member of, ApplicantMember Phone Number, ApplicantMember Signature, Date, NOTE The application may not be, Department of Human Services DHS, AUTHORITY, PA of, COMPLETION, Mandatory, NONCOMPLETION, License issuance will be denied, and BCAL Rev Previous edition will finalize the process and you'll be done before you know it!
Step 3: Prior to finishing your document, you should make sure that all blanks were filled in the correct way. Once you’re satisfied with it, click on “Done." Find the aged application printable as soon as you register at FormsPal for a 7-day free trial. Readily access the pdf file within your personal account, with any edits and adjustments automatically preserved! FormsPal is dedicated to the privacy of our users; we make sure all information handled by our system is kept secure.