
C-1 can be filled in online with ease. Simply open FormsPal PDF editing tool to get the job done quickly. FormsPal professional team is always working to enhance the tool and make it much better for users with its cutting-edge features. Take your experience to a higher level with constantly improving and exciting possibilities available today! With a few simple steps, you'll be able to begin your PDF editing:
Step 1: First, open the pdf tool by clicking the "Get Form Button" above on this site.
Step 2: With the help of our state-of-the-art PDF editor, it's possible to accomplish more than simply fill out blank form fields. Try all the functions and make your forms appear faultless with custom text added in, or fine-tune the file's original input to perfection - all comes along with an ability to add any type of photos and sign the file off.
This document requires some specific information; to guarantee correctness, be sure to adhere to the subsequent suggestions:
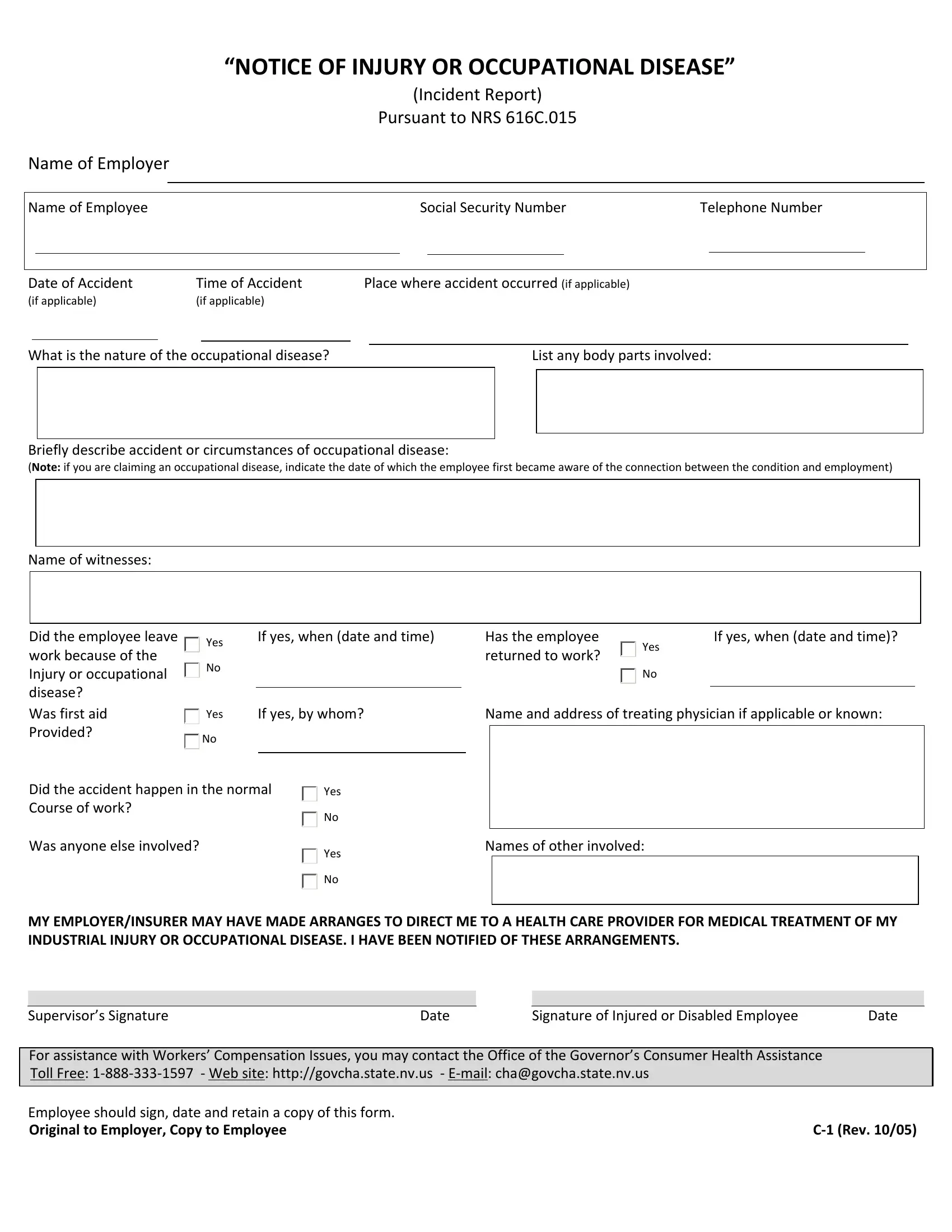
1. It's vital to complete the C-1 accurately, thus be attentive while filling in the sections including these blanks:
2. Once your current task is complete, take the next step – fill out all of these fields - Did the employee leave work, Was first aid Provided, Yes, Yes, If yes when date and time, Has the employee returned to work, Yes, If yes when date and time, If yes by whom, Name and address of treating, Did the accident happen in the, Was anyone else involved, Yes, Yes, and Names of other involved with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
Those who work with this form generally make errors while filling out Yes in this part. Remember to go over whatever you enter right here.
Step 3: Go through the information you have entered into the form fields and press the "Done" button. After setting up afree trial account at FormsPal, you will be able to download C-1 or email it directly. The PDF file will also be accessible through your personal account with your each edit. FormsPal ensures your data confidentiality with a protected system that in no way records or shares any type of personal data involved. Be confident knowing your documents are kept safe when you use our editor!