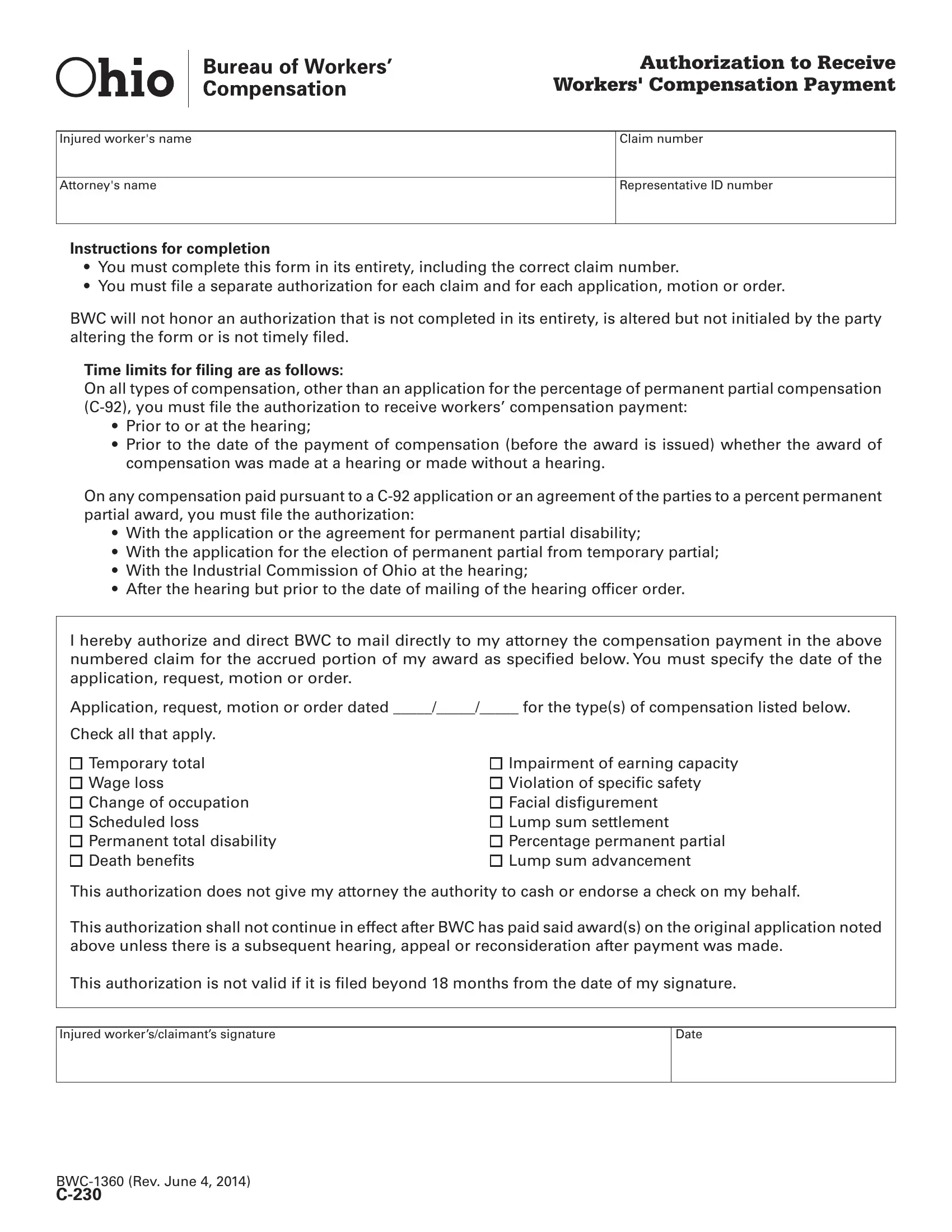
When navigating the intricacies of receiving workers' compensation payments in Ohio, one critical piece of documentation stands out: the C-230 form, officially termed as "Authorization to Receive Workers' Compensation Payment." This essential form serves a vital function by authorizing the direct mailing of compensation payments to an attorney, on behalf of an injured worker. The comprehensive form requires detailed information including the injured worker's name, attorney’s name, claim number, and representative ID number, ensuring that all necessary parties are correctly identified. Furthermore, the form mandates that every section be completed in full, emphasizing the need for accuracy and completeness, with a specific insistence on the inclusion of the correct claim number. It outlines explicit instructions regarding filing times for different types of compensation claims, highlighting the necessity of timely submission to avoid forfeiture of rights to compensation. The form facilitates various compensation types, ranging from temporary total disability to death benefits, and explicitly states that it does not grant the attorney the power to cash or endorse the compensation check. This vital document, while simple in its essence, plays a crucial role in the workers' compensation process, ensuring that the legal representatives can efficiently manage the compensation awarded to injured workers, within the boundaries of Ohio’s workers' compensation system regulations.
| Question | Answer |
|---|---|
| Form Name | Form C 230 Ohio |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | initialed, disfigurement, C-230, BWC |
Authorization to Receive Workers' Compensation Payment
Injured worker's name
Attorney's name
Claim number
Representative ID number
Instructions for completion
•You must complete this form in its entirety, including the correct claim number.
•You must file a separate authorization for each claim and for each application, motion or order.
BWC will not honor an authorization that is not completed in its entirety, is altered but not initialed by the party altering the form or is not timely filed.
Time limits for filing are as follows:
On all types of compensation, other than an application for the percentage of permanent partial compensation
•Prior to or at the hearing;
•Prior to the date of the payment of compensation (before the award is issued) whether the award of compensation was made at a hearing or made without a hearing.
On any compensation paid pursuant to a
•With the application or the agreement for permanent partial disability;
•With the application for the election of permanent partial from temporary partial;
•With the Industrial Commission of Ohio at the hearing;
•After the hearing but prior to the date of mailing of the hearing officer order.
I hereby authorize and direct BWC to mail directly to my attorney the compensation payment in the above numbered claim for the accrued portion of my award as specified below. You must specify the date of the application, request, motion or order.
Application, request, motion or order dated _____/_____/_____ for the type(s) of compensation listed below.
Check all that apply.
Temporary total |
Impairment of earning capacity |
Wage loss |
Violation of specific safety |
Change of occupation |
Facial disfigurement |
Scheduled loss |
Lump sum settlement |
Permanent total disability |
Percentage permanent partial |
Death benefits |
Lump sum advancement |
This authorization does not give my attorney the authority to cash or endorse a check on my behalf.
This authorization shall not continue in effect after BWC has paid said award(s) on the original application noted above unless there is a subsequent hearing, appeal or reconsideration after payment was made.
This authorization is not valid if it is filed beyond 18 months from the date of my signature.
Injured worker’s/claimant’s signature
Date