
c4 compensation can be filled in online in no time. Simply open FormsPal PDF tool to perform the job right away. Our editor is consistently developing to grant the best user experience attainable, and that's due to our resolve for continual enhancement and listening closely to feedback from customers. All it takes is just a few easy steps:
Step 1: Firstly, open the pdf tool by pressing the "Get Form Button" in the top section of this page.
Step 2: With our state-of-the-art PDF editing tool, you're able to accomplish more than merely complete blank fields. Try all the features and make your forms appear faultless with custom textual content added in, or optimize the original input to perfection - all that comes along with an ability to insert your personal photos and sign it off.
It really is straightforward to complete the document with our practical guide! Here is what you need to do:
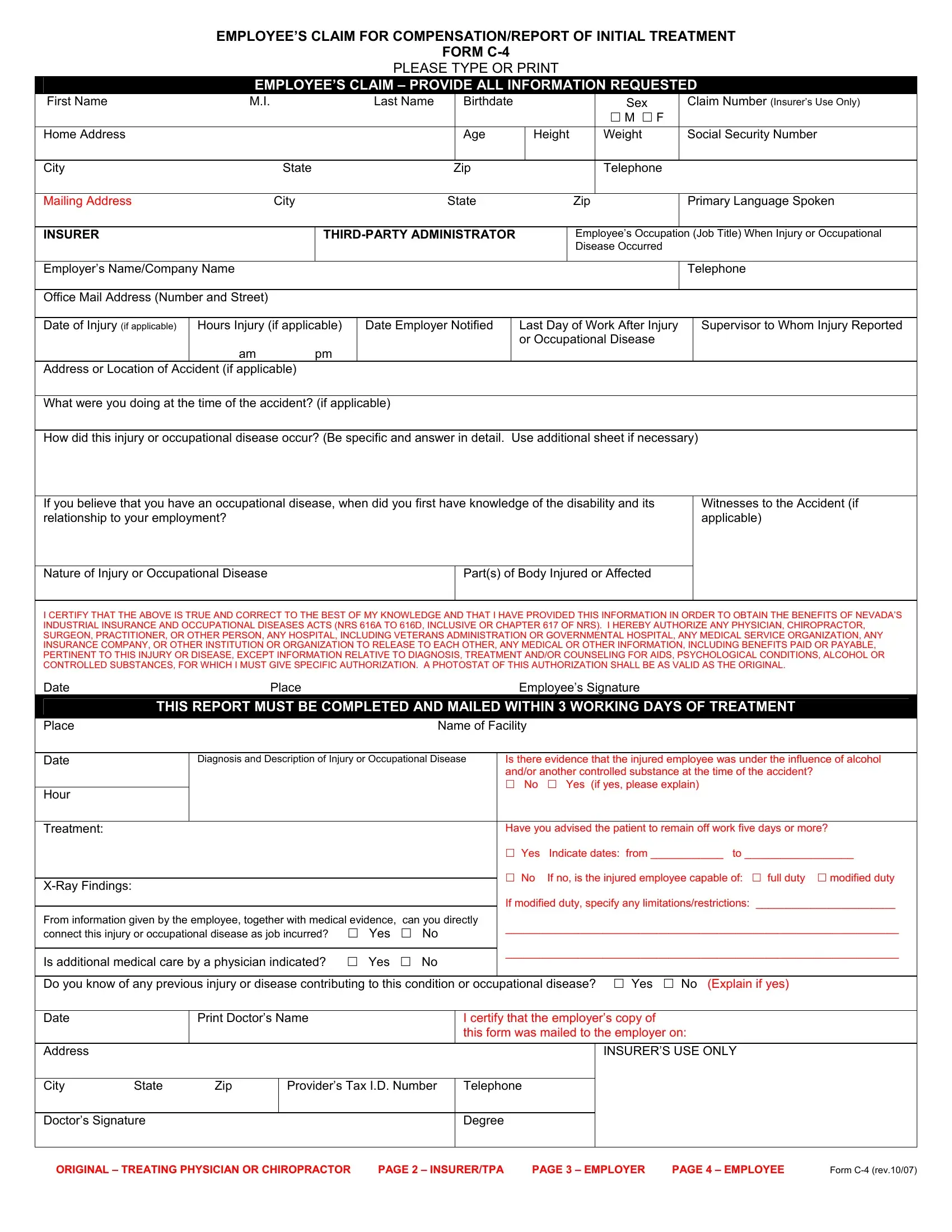
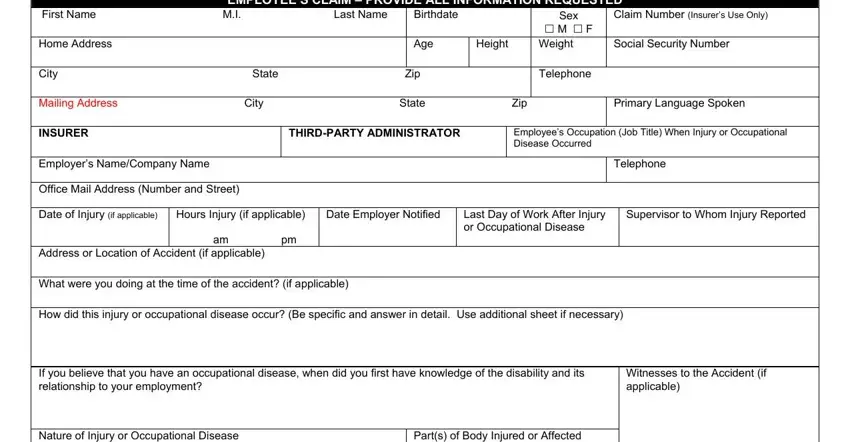
1. The c4 compensation requires certain information to be inserted. Ensure that the next blank fields are finalized:
2. Once your current task is complete, take the next step – fill out all of these fields - I CERTIFY THAT THE ABOVE IS TRUE, THIS REPORT MUST BE COMPLETED AND, Place Name of Facility, Diagnosis and Description of, Is there evidence that the injured, Date, Hour, Treatment, XRay Findings, Have you advised the patient to, cid Yes Indicate dates from to, cid No If no is the injured, If modified duty specify any, From information given by the, and Is additional medical care by a with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
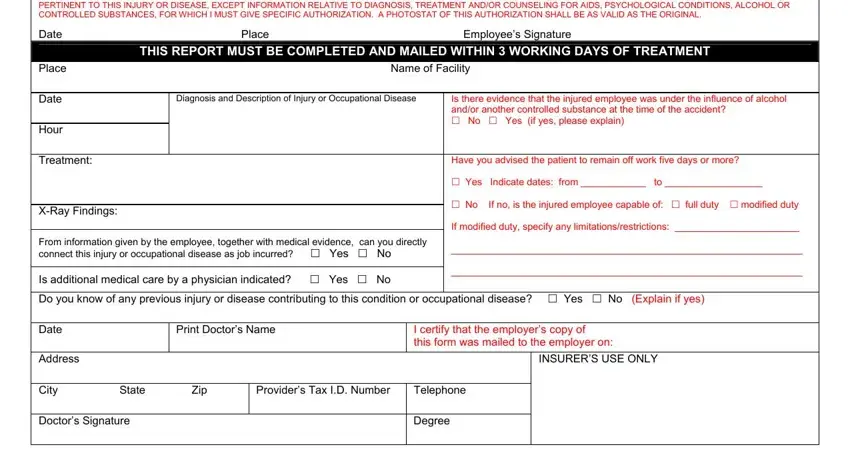
People often make some mistakes while filling out THIS REPORT MUST BE COMPLETED AND in this part. You should definitely re-examine what you enter right here.
Step 3: As soon as you've glanced through the information in the blanks, simply click "Done" to finalize your document creation. Right after registering afree trial account with us, you'll be able to download c4 compensation or email it immediately. The document will also be easily accessible through your personal account with all your changes. We do not sell or share any information you provide while working with documents at FormsPal.