Managing forms using our PDF editor is simpler than anything. To edit c4 2 form the document, you'll find nothing you should do - only continue with the steps below:
Step 1: Look for the button "Get Form Here" on the following site and next, click it.
Step 2: When you enter the c4 2 form editing page, you will see lots of the functions you can undertake regarding your document within the upper menu.
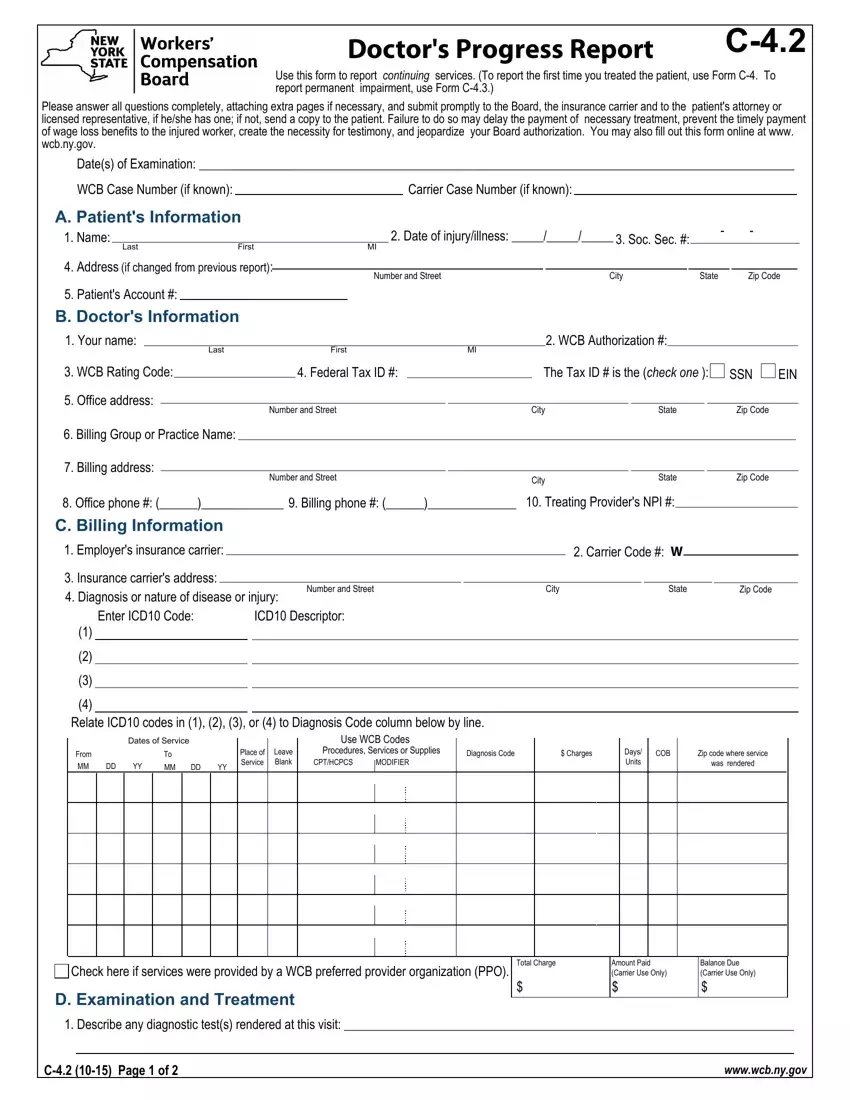
Prepare the c4 2 form PDF by entering the data needed for each individual part.
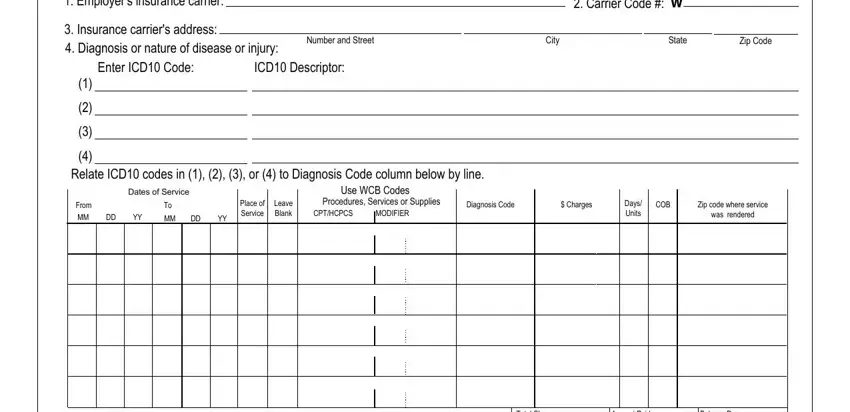
Put the demanded details in the Employers insurance carrier, Insurance carriers address, Number and Street, City, State, Zip Code, Carrier Code W, Enter ICD Code, ICD Descriptor, Relate ICD codes in or to, Dates of Service, From MM DD YY, MM DD YY, Place of Service, and Leave Blank field.
Within the segment talking about Check here if services were, D Examination and Treatment, Total Charge, Amount Paid Carrier Use Only, Balance Due Carrier Use Only, Describe any diagnostic tests, C Page of, and wwwwcbnygov, you have got to note some required information.

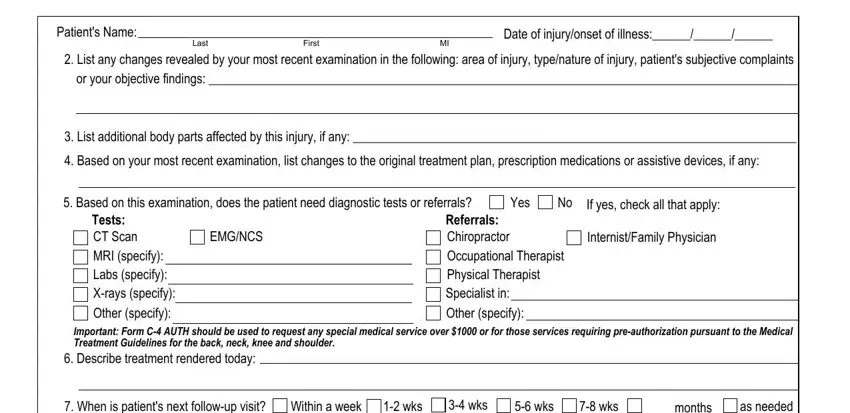
The Patients Name, Last First MI, Date of injuryonset of illness, List any changes revealed by your, List additional body parts, Based on your most recent, Based on this examination does, Yes, If yes check all that apply, EMGNCS, Tests CT Scan MRI specify Labs, InternistFamily Physician, Referrals Chiropractor, Important Form C AUTH should be, and Describe treatment rendered today section is the place to put the rights and obligations of all parties.
Check the areas E Doctors Opinion based on this, In your opinion was the incident, Yes Yes, No No, Yes, NA no findings at this time, What is the percentage of, Describe findings and relevant, F Return to Work Is patient, Yes, If yes are there work restrictions, Yes, If yes describe the work, How long will the work, and days and next fill them in.
Step 3: Press "Done". Now you may export the PDF file.
Step 4: To stay away from potential upcoming concerns, ensure you possess at the very least a few copies of each separate document.
