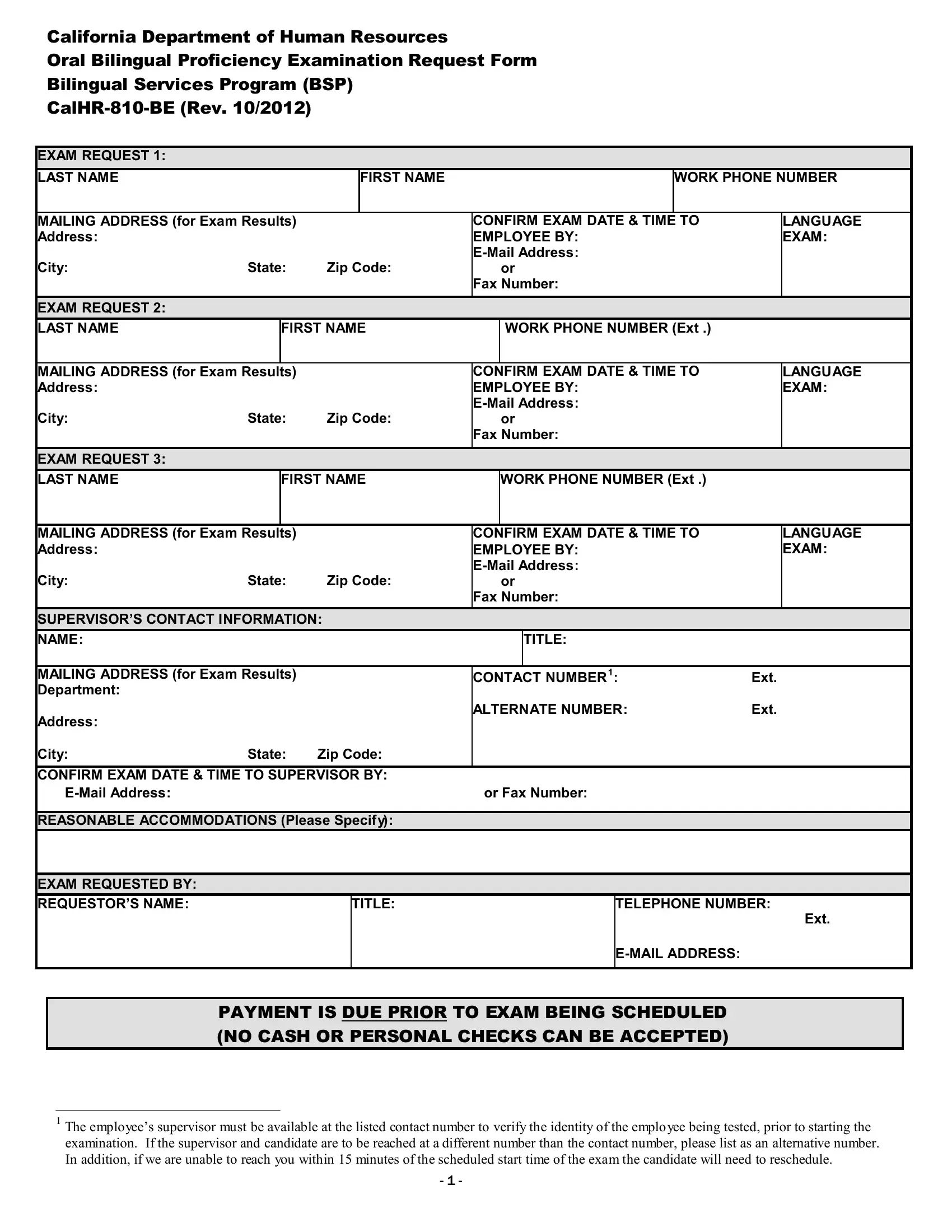
In today's global and multicultural work environment, the ability to communicate effectively in multiple languages is highly valued. Recognizing this importance, the California Department of Human Resources provides a mechanism for certifying bilingual proficiency among employees through the CalHR-810-BE form, part of the Bilingual Services Program (BSP). This form serves as a request for an Oral Bilingual Proficiency Examination, a crucial step for employees who need to demonstrate their ability to communicate effectively in languages other than English. Given its significance, the form includes detailed sections for exam requests, including personal and contact information for the employee and their supervisor, the language of the exam, and preferred contact methods for confirming the exam date and time. It also outlines the requirements for payment prior to the examination, offering several payment methods for the exam fee, which emphasizes the structured and accessible approach the department aims to provide. Furthermore, it addresses the need for reasonable accommodations, ensuring that all employees have a fair opportunity to showcase their language proficiency. This intricate process, outlined by the CalHR-810-BE form, reflects the department's commitment to fostering a diverse and inclusive workforce capable of serving the state's multilingual population.
| Question | Answer |
|---|---|
| Form Name | Form Calhr 810 Be |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CalHR 810 BE calhr bilingual exams form |
California Department of Human Resources
Oral Bilingual Proficiency Examination Request Form
Bilingual Services Program (BSP)
EXAM REQUEST 1:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
|
|
|
|
|
FIRST NAME |
|
|
|
|
WORK PHONE NUMBER |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MAILING ADDRESS (for Exam Results) |
|
|
|
CONFIRM EXAM DATE & TIME |
TO |
|
LANGUAGE |
|
|||||||
|
Address: |
|
|
|
|
|
|
|
EMPLOYEE BY: |
|
EXAM: |
|
||||
|
City: |
State: |
Zip Code: |
|
|
|
||||||||||
|
|
or |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
Fax Number: |
|
|
|
||||
|
EXAM REQUEST 2: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
FIRST NAME |
|
WORK PHONE NUMBER (Ext .) |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
MAILING ADDRESS (for Exam Results) |
|
|
|
CONFIRM EXAM DATE & TIME TO |
|
LANGUAGE |
|
||||||||
|
Address: |
|
|
|
|
|
|
|
EMPLOYEE BY: |
|
EXAM: |
|
||||
|
City: |
State: |
Zip Code: |
|
|
|
||||||||||
|
|
or |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
Fax Number: |
|
|
|
||||
|
EXAM REQUEST 3: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LAST NAME |
|
|
|
FIRST NAME |
|
WORK PHONE NUMBER (Ext .) |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
MAILING ADDRESS (for Exam Results) |
|
|
|
CONFIRM EXAM DATE & TIME TO |
|
LANGUAGE |
|
||||||||
|
Address: |
|
|
|
|
|
|
|
EMPLOYEE BY: |
|
EXAM: |
|
||||
|
City: |
State: |
Zip Code: |
|
|
|
||||||||||
|
|
or |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
Fax Number: |
|
|
|
||||
|
SUPERVISOR’S CONTACT INFORMATION: |
|
|
|
|
|
|
|
|
|||||||
|
NAME: |
|
|
|
|
|
|
|
|
|
TITLE: |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|||||||
|
MAILING ADDRESS (for Exam Results) |
|
|
|
CONTACT NUMBER1: |
Ext. |
|
|||||||||
|
Department: |
|
|
|
|
|
|
|
ALTERNATE NUMBER: |
Ext. |
|
|||||
|
Address: |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
State: |
Zip Code: |
|
|
|
|
|
|
|
|
|||||
|
CONFIRM EXAM DATE & TIME TO SUPERVISOR BY: |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
or Fax Number: |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
||||||
|
REASONABLE ACCOMMODATIONS (Please Specify): |
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXAM REQUESTED BY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REQUESTOR’S NAME: |
|
|
|
|
|
TITLE: |
|
|
|
TELEPHONE NUMBER: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ext. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAYMENT IS DUE PRIOR TO EXAM BEING SCHEDULED (NO CASH OR PERSONAL CHECKS CAN BE ACCEPTED)
1The employee’s supervisor must be available at the listed contact number to verify the identity of the employee being tested, prior to starting the examination. If the supervisor and candidate are to be reached at a different number than the contact number, please list as an alternative number. In addition, if we are unable to reach you within 15 minutes of the scheduled start time of the exam the candidate will need to reschedule.
-1 -
California Department of Human Resources
Oral Bilingual Proficiency Examination Request Form
Bilingual Services Program (BSP)
|
PAYMENT METHOD: |
|
|
|
|
|
|
|
|
|
|
Mail Payment & Request Form To: |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
$115.00/ea. - Purchase/Service Order # |
|
|
(Attached) |
|
CalHR – Office of Civil Rights |
|||||||||
* |
|
|
|
|
|
|
|
|
|
|
|
||||
|
$115.00/ea. - Bill Consolidated Contract # |
|
|
|
* |
|
|
Bilingual Services Program |
|||||||
|
|
|
|||||||||||||
|
$115.00/ea. – Cashier’s Check or Money Order Enclosed |
|
Attn: Bilingual Testing Coordinator |
||||||||||||
|
|
1515 S Street, North Bldg., Ste. 400 |
|||||||||||||
|
(California Department of Human Resources) |
|
|||||||||||||
|
$115.00/ea. – Cal Card or Credit Card* |
|
|
|
|
|
|
Sacramento, CA |
|||||||
|
|
|
|
|
|
|
For Information or Questions: |
||||||||
|
|
x$_ |
=$ |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
(916) |
|
||||||
|
# of Exams |
Cost Per Exam |
Total Cost |
|
|
||||||||||
|
|
Fax: (916) |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|||||||||
|
*IF PAYING BY CONSOLIDATED CONTRACT OR PURCHASE/SERVICE ORDER, PLEASE INCLUDE THE FOLLOWING |
|
|||||||||||||
|
INFORMATION. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of person to invoice: |
|
|
|
|
|
|
Unit: |
|
|
|||||
|
Address: |
|
|
|
|
City: |
|
State: |
Zip Code: |
||||||
|
Phone number: |
|
|
|
|
|
|
|
|
Fax number: |
|
|
|||
|
*IF PAYING BY CREDIT CARD/CAL CARD: |
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
||||||||
|
Name of the Candidate(s) for which this payment should be applied: |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Number of Exams |
|
Item Description |
|
|
Cost Per Item |
Total Cost to be Charged |
|
|||||||
|
|
|
|
Bilingual Oral Fluency |
|
$115.00 |
|
|
|||||||
|
|
|
|
|
Examination |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
Credit Card |
Information |
|
|
||||
|
Name of Card Holder (as it appears on the credit card): |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|||||||||
|
Type of Credit Card: |
Cal Card |
Visa |
MasterCard |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Credit Card #: |
|
|
|
|
|
|
Expiration Date: |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Mailing Address (to send receipt): |
|
|
|
|
|
|
|
|
|
|||||
|
Address: |
|
|
|
|
|
City: |
|
State: |
Zip: |
|||||
Contact Telephone Number:
I Hereby Authorize the Department of Human Resources to charge my credit card for the total cost of administering the above bilingual oral fluency exam(s).
Signature of Card Holder:
THE EMPLOYEE AND SUPERVISOR WILL RECEIVE CONFIRMATION BY
I hereby certify that I am authorized to submit a request for bilingual fluency examination, as or on behalf of, the department’s testing officer.
Signed: |
Title: |
Date: |
|
|
|
- 2 -