
Dealing with PDF documents online can be super easy with our PDF tool. You can fill out PID here within minutes. The editor is consistently upgraded by us, receiving handy features and becoming even more versatile. Starting is easy! All that you should do is stick to the next easy steps down below:
Step 1: Firstly, access the tool by clicking the "Get Form Button" at the top of this site.
Step 2: As soon as you start the online editor, you'll see the form prepared to be filled out. Besides filling in various blanks, you might also perform other actions with the form, particularly writing any words, editing the initial text, inserting images, signing the form, and much more.
This PDF form will need some specific information; to ensure accuracy and reliability, please make sure to take note of the recommendations just below:
1. You need to fill out the PID accurately, thus be attentive when filling in the parts containing all of these blank fields:
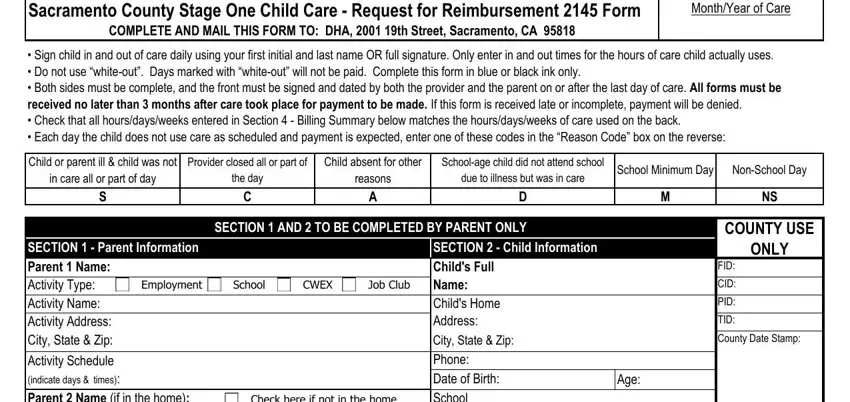
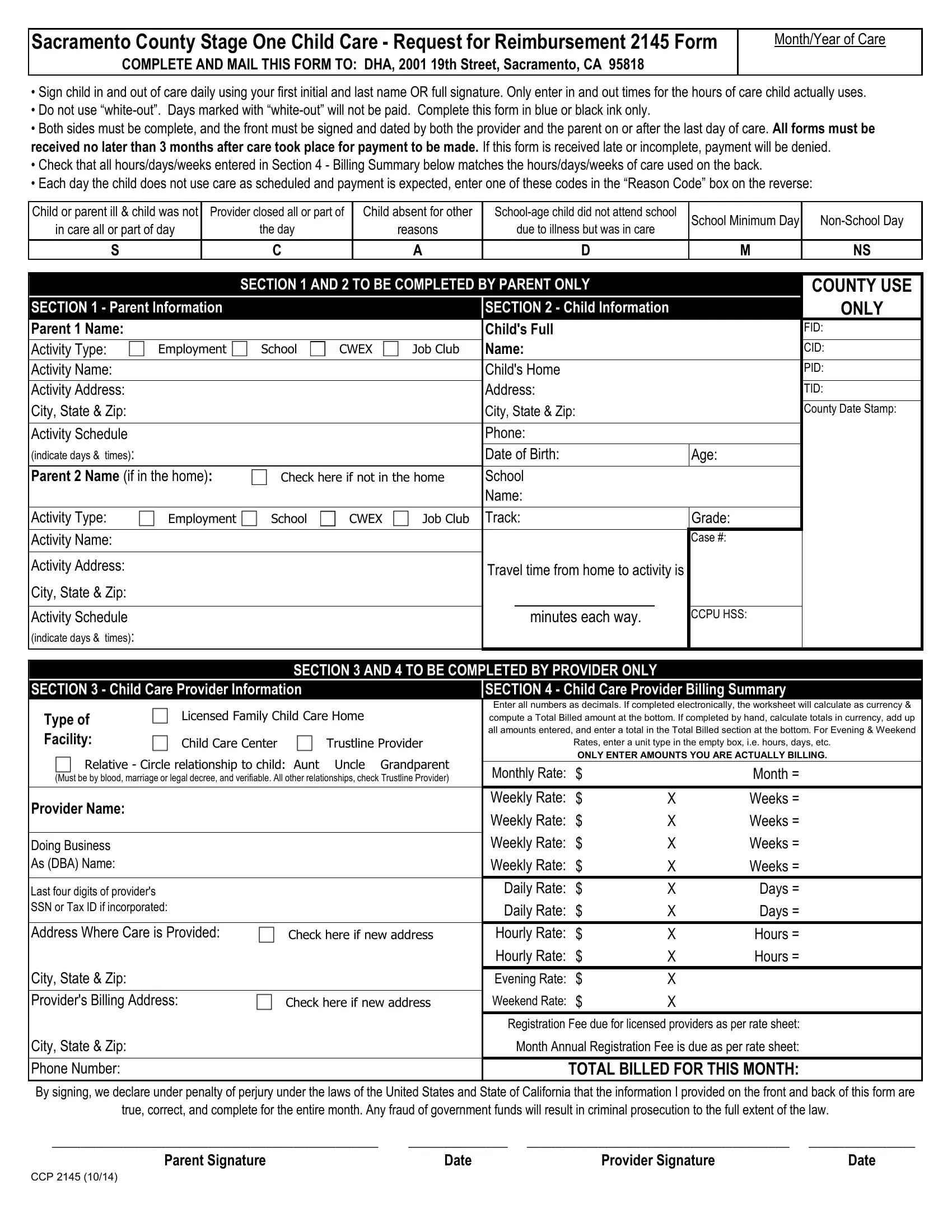
2. Once your current task is complete, take the next step – fill out all of these fields - SECTION Parent Information, Check here if not in the home, Employment, School, CWEX, Job Club, Activity Type Activity Name, Activity Address, City State Zip, Activity Schedule indicate days, Childs Full Name Childs Home, Grade Case, Travel time from home to activity, minutes each way, and CCPU HSS with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
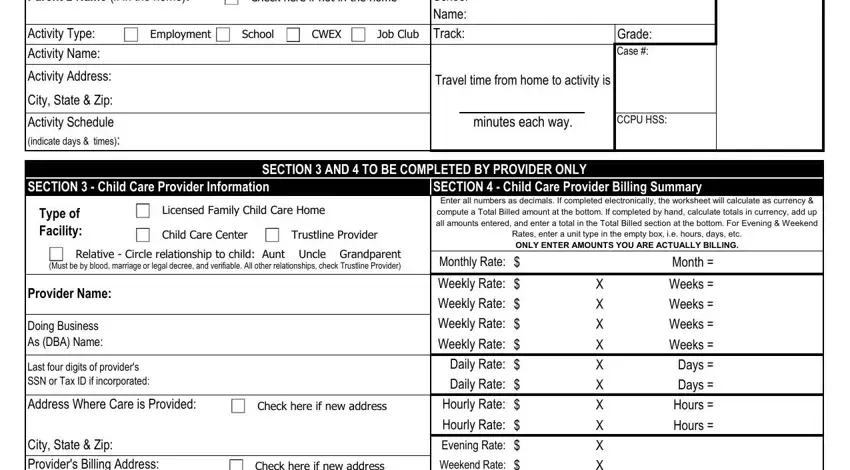
3. This third section should also be fairly simple, City State Zip Providers Billing, City State Zip Phone Number, Check here if new address, Weekend Rate, X X X X X X X X X X, Registration Fee due for licensed, Month Annual Registration Fee is, TOTAL BILLED FOR THIS MONTH, By signing we declare under, true correct and complete for the, Parent Signature, Date, Provider Signature, Date, and CCP - all of these blanks will need to be filled out here.
People who use this PDF generally make some errors when filling out Check here if new address in this part. Be sure you read again whatever you enter right here.
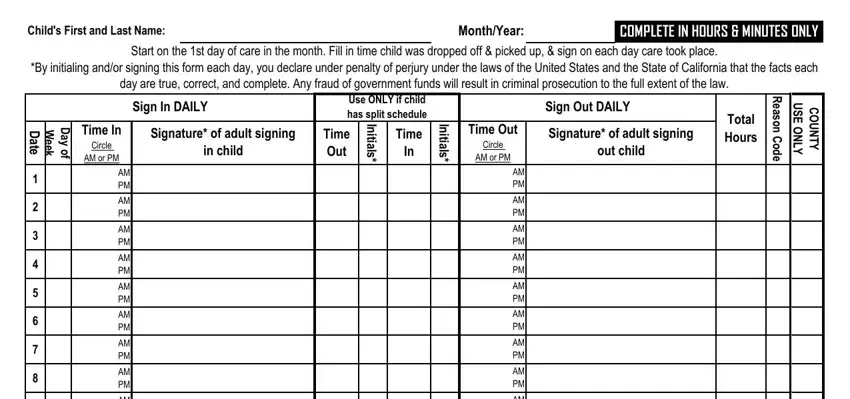
4. You're ready to complete this next part! In this case you'll get all these Childs First and Last Name, MonthYear, COMPLETE IN HOURS MINUTES ONLY, Start on the st day of care in the, By initialing andor signing this, day are true correct and complete, Sign In DAILY, Use ONLY if child has split, Sign Out DAILY, D a t e, W e e k, D a y o f, Time In, Circle, and AM or PM fields to do.
5. Finally, the following final section is precisely what you will need to finish prior to submitting the form. The fields under consideration are the next: AM PM, AM PM, AM PM, AM PM, AM PM, AM PM, AM PM, AM PM, AM PM, AM PM, AM PM, AM PM, AM PM, AM PM, and AM PM.
Step 3: Check the information you have typed into the form fields and then hit the "Done" button. Join FormsPal now and instantly get access to PID, ready for download. Every edit you make is handily kept , which enables you to change the document at a later point if necessary. FormsPal offers secure form completion with no personal data record-keeping or any sort of sharing. Rest assured that your information is safe with us!