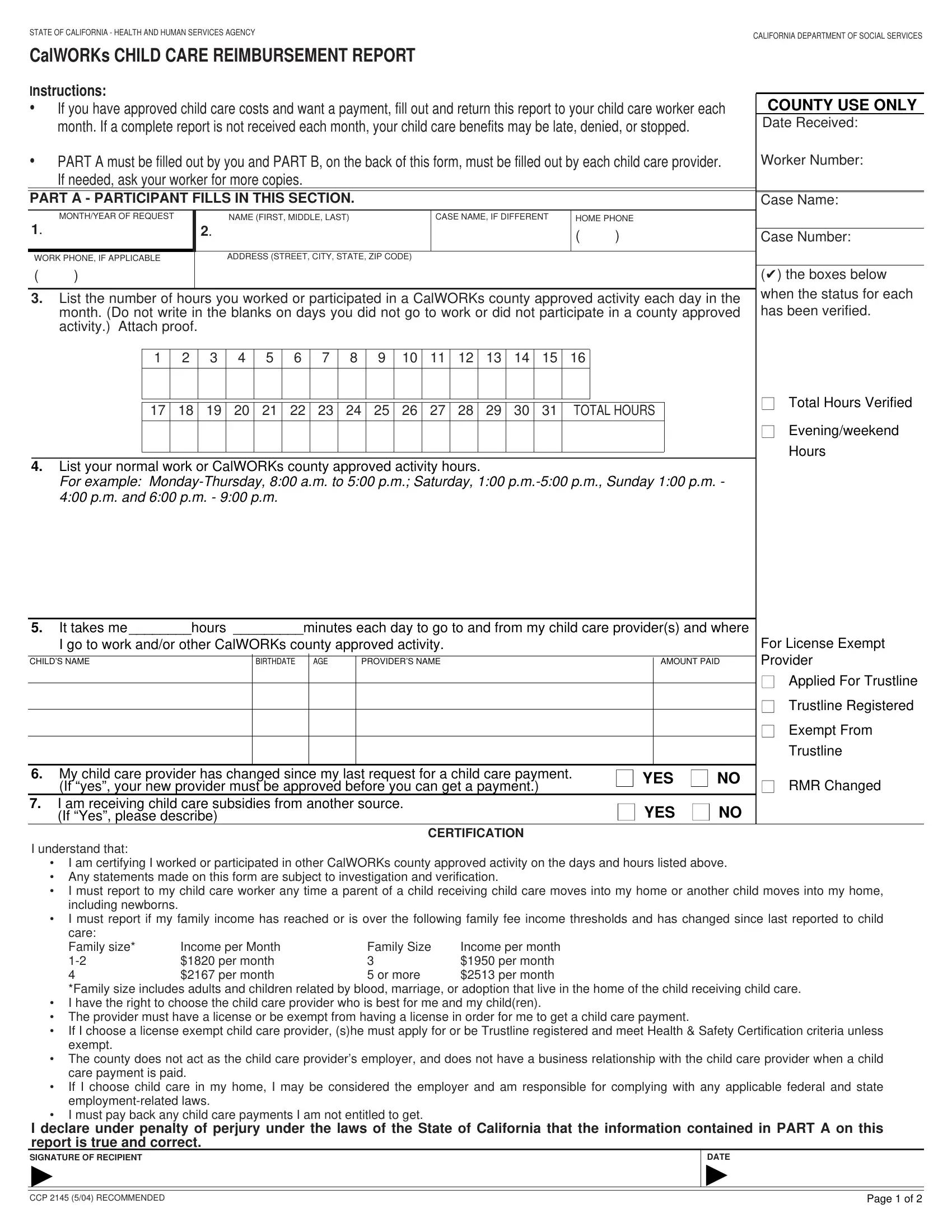
Navigating the intricacies of child care assistance under the California Work Opportunity and Responsibility to Kids (CalWORKs) program can be complex, but the CCP 2145 form serves as a crucial tool for families seeking reimbursement for child care expenses. This comprehensive form, issued by the State of California Health and Human Services Agency and managed by the California Department of Social Services, is designed to streamline the reporting process for both participants and child care providers. With its dual-part structure, the form requires detailed information about child care services rendered, including hours of care provided, the cost of care, and the provider’s licensing status, among other vital data. Part A of the form is filled out by the CalWORKs participant, where they detail their work or activity hours and child care needs, while Part B is completed by the child care provider, offering a transparent account of the services offered. This meticulous documentation is critical not only for ensuring accurate reimbursement but also for upholding the integrity of the child care support system. Moreover, the form contains explicit instructions for reporting changes in the provider or the recipient's circumstances, emphasizing the importance of updated and accurate information. It encapsulates a robust mechanism for verifying care provision and enables participants to exercise their right to select a suitable child care provider, ensuring that the assistance provided aligns with the welfare and developmental needs of children and the economic realities of their families.
| Question | Answer |
|---|---|
| Form Name | From Ccp 2145 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CHILDS, RMR, CALIFORNIA, familys |