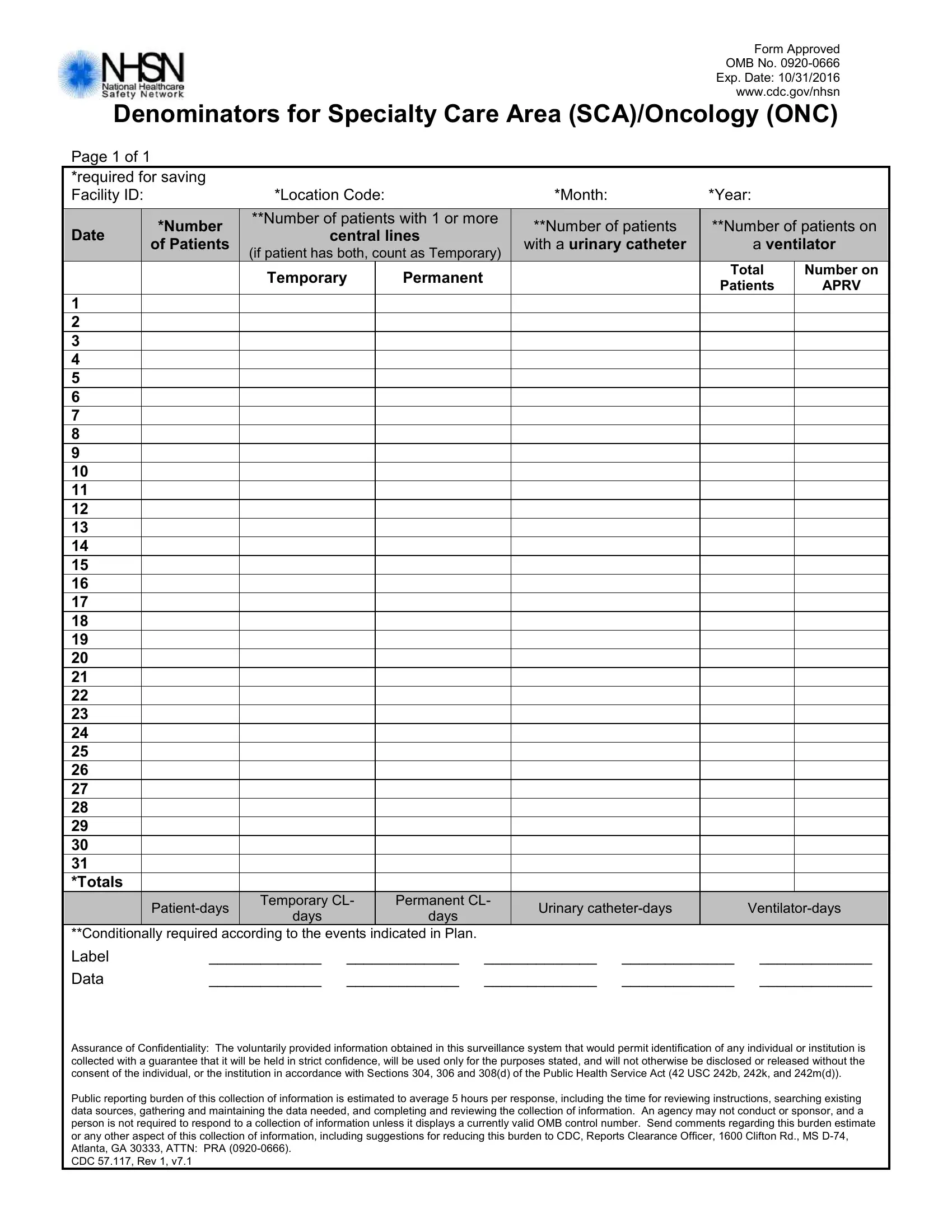
In the realm of healthcare, accurate data collection and reporting are pivotal for enhancing patient care and oversight. The CDC 57 117 form serves as a critical tool in this endeavor, particularly for Specialty Care Areas (SCA) and Oncology units. This document, officially recognized and mandated under OMB No. 0920-0666 with an expiration date of October 31, 2016, is structured to meticulously gather monthly data on various patient care metrics. Essential elements captured include the number of patients with central lines, those with urinary catheters, and those requiring ventilator support, distinguishing between temporary and permanent situations. Facilities are required to report not just patient numbers but also the days each device was used, offering a comprehensive view of the care environment. Beyond mere numbers, the form ensures confidentiality, abiding by Sections 304, 306, and 308(d) of the Public Health Service Act, thus promising the safeguarding of personal and institutional data. It underscores the public reporting burden estimated at 5 hours per response, acknowledging the effort necessary for compliance but emphasizing the value of the information collected. By completing this form, healthcare providers contribute to a larger database, managed by the CDC's National Healthcare Safety Network (NHSN), aimed at monitoring and improving quality care standards across the nation.
| Question | Answer |
|---|---|
| Form Name | Form Cdc 57 117 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 242b, Exp, D-74, 242k |
Form Approved
OMB No.
Exp. Date: 10/31/2016
www.cdc.gov/nhsn
Denominators for Specialty Care Area (SCA)/Oncology (ONC)
Page 1 of 1
|
|
*required for saving |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Facility ID: |
|
|
|
*Location Code: |
|
|
|
|
*Month: |
|
|
*Year: |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
**Number of patients with 1 or more |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Date |
|
|
*Number |
|
|
|
**Number of patients |
|
|
**Number of patients on |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
central lines |
|
|
|
|||||||||||||
|
|
|
|
of Patients |
|
|
|
|
|
|
with a urinary catheter |
|
|
|
a ventilator |
|
|
||||||
|
|
|
|
|
|
|
(if patient has both, count as Temporary) |
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
Temporary |
|
Permanent |
|
|
|
|
|
|
|
Total |
Number on |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patients |
APRV |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
23 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
25 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
26 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
27 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
28 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
29 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Totals |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Temporary CL- |
|
Permanent CL- |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
Urinary |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
days |
|
|
days |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
**Conditionally required according to the events indicated in Plan. |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Label |
_____________ |
_____________ |
_____________ |
_____________ |
_____________ |
|
|
||||||||||||||
|
|
Data |
_____________ |
_____________ |
_____________ |
_____________ |
_____________ |
|
|
||||||||||||||
Assurance of Confidentiality: The voluntarily provided information obtained in this surveillance system that would permit identification of any individual or institution is collected with a guarantee that it will be held in strict confidence, will be used only for the purposes stated, and will not otherwise be disclosed or released without the consent of the individual, or the institution in accordance with Sections 304, 306 and 308(d) of the Public Health Service Act (42 USC 242b, 242k, and 242m(d)).
Public reporting burden of this collection of information is estimated to average 5 hours per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. An agency may not conduct or sponsor, and a person is not required to respond to a collection of information unless it displays a currently valid OMB control number. Send comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden to CDC, Reports Clearance Officer, 1600 Clifton Rd., MS
CDC 57.117, Rev 1, v7.1